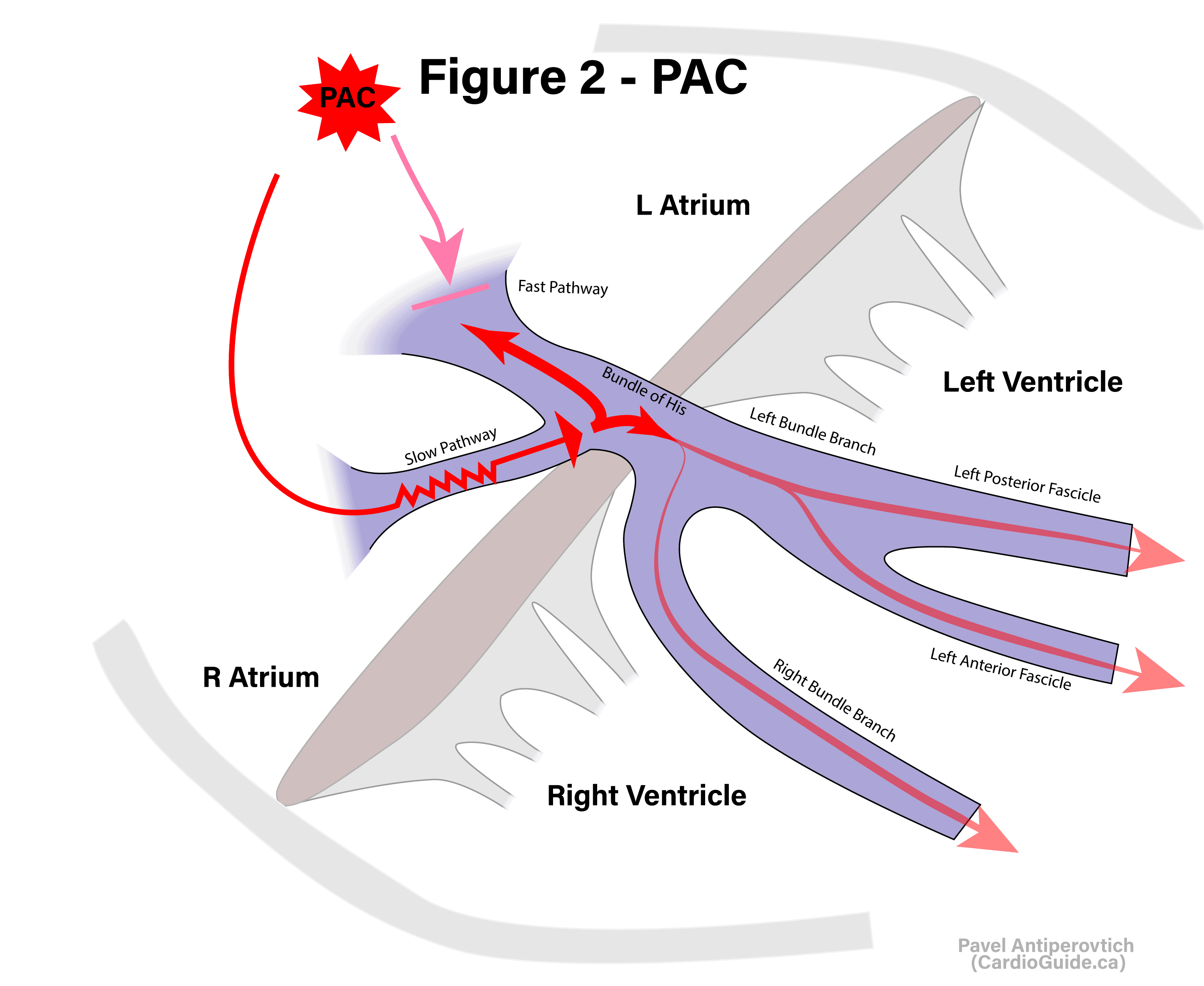
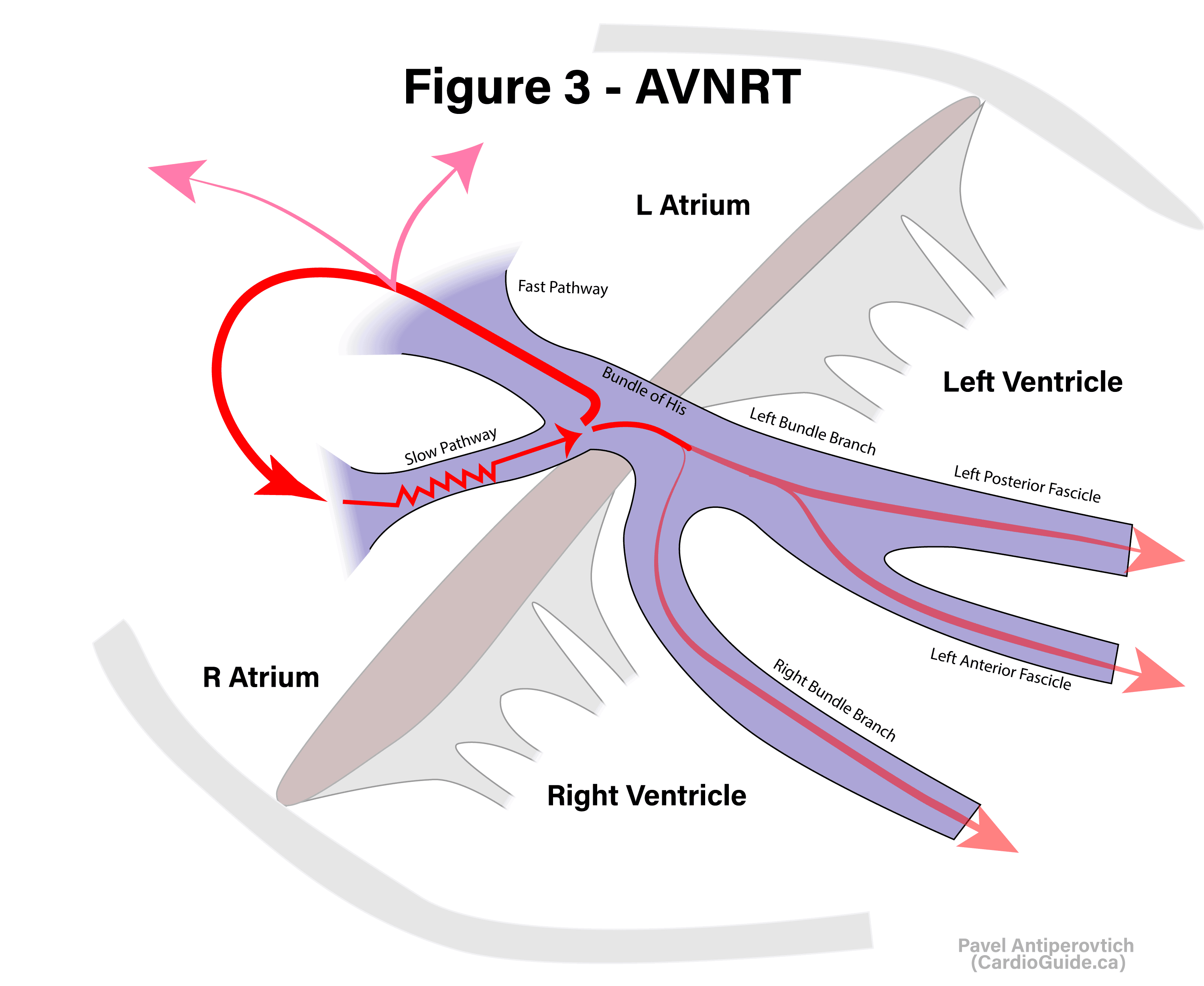
Slow-Fast “Typical” AVNRT: On occasion, a specially-timed PAC can reach the AV node at a vulnerable time period, such that the fast pathway is refractory. It then enters the node via the slow pathway (Figure 2). By the time it reaches the common fibres, the fast pathway recovers. The signal goes down to activate the ventricles, and at the same time retro-conducts up via fast pathway to the atria, which activates the slow pathway again resulting in a macro-reentry circuit. This is slow-fast “typical” AVNRT.









{kind=link}
{kind=link}
{kind=link}