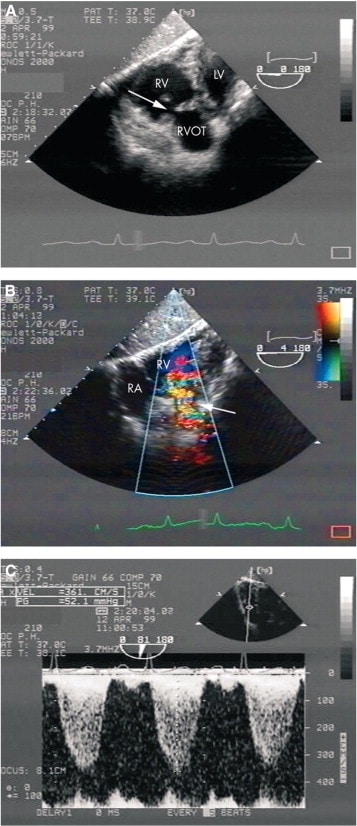
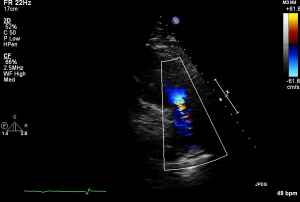
- History of carcinoid heart disease with previous tricuspid replacement
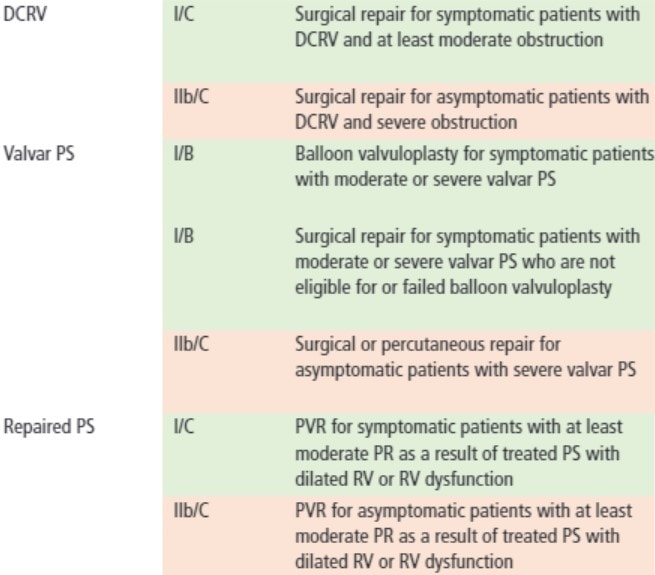
- Progressive pulmonary stenosis and shortness of breath
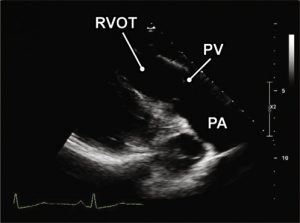
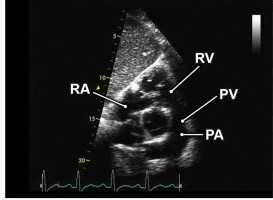
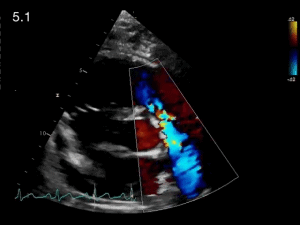
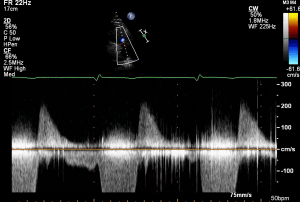
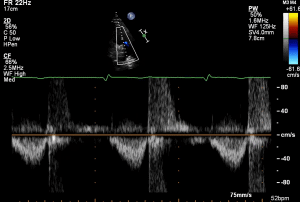
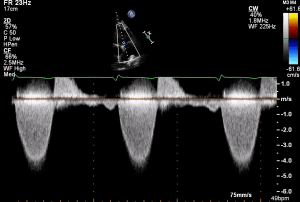
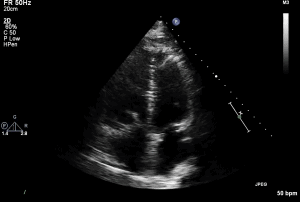
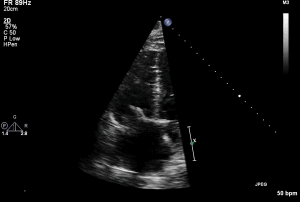
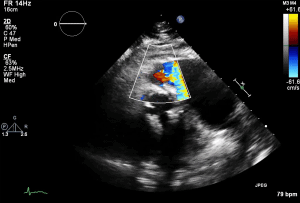
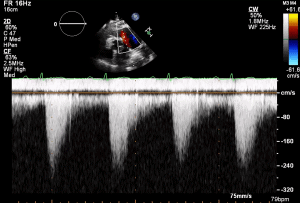
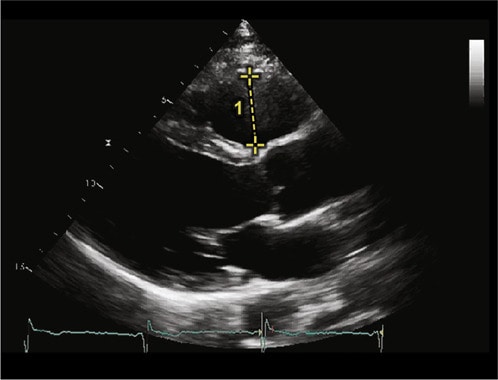
- TTE shown 1 day prior to pulmonary valve replacement
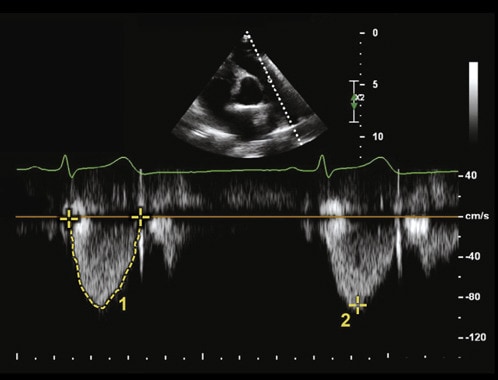
- Severe PS with max velocity 4.6m/s and mean gradient 84.6mmHg
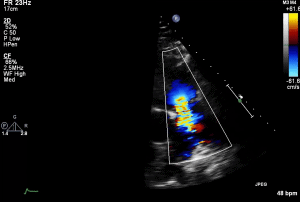
- Moderate PR
- Mod-Severe RV dysfunction
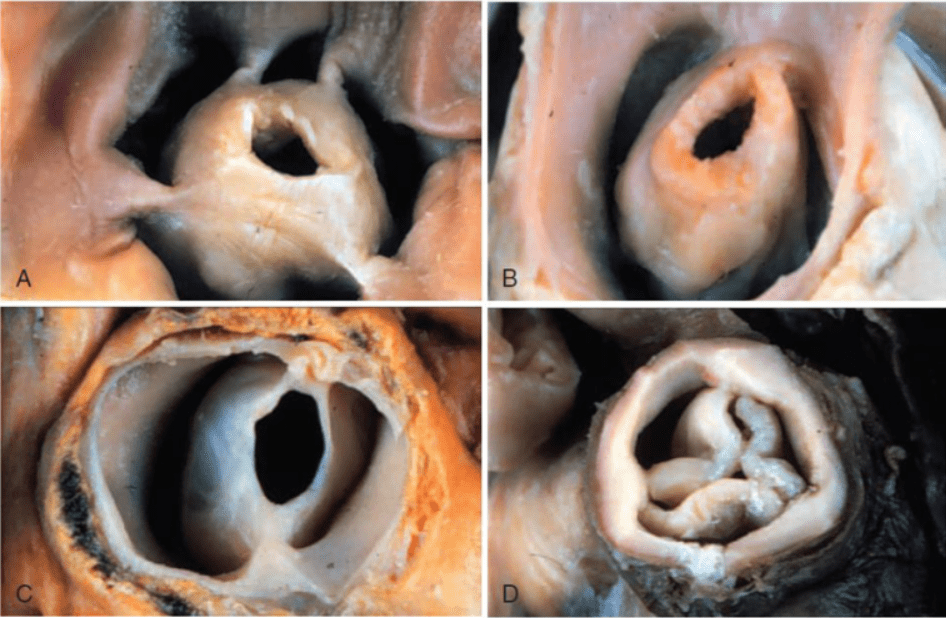
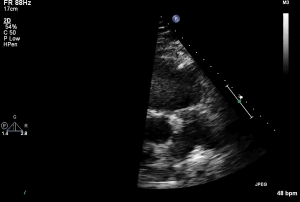
- Carcinoid involvement of pulmonic valve classically showed thickened valve with restricted motion
Thank you Dr. Dias and Diamantouros for the case.

{kind=link}
{kind=link}
{kind=link}
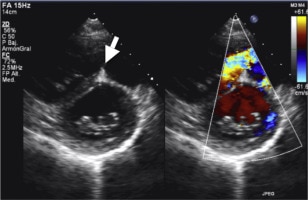
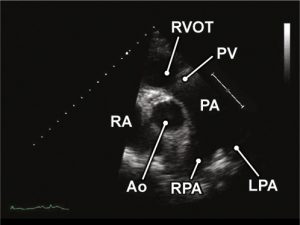
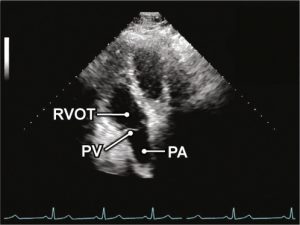
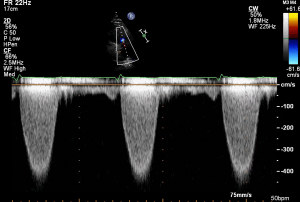
- History of rheumatic heart disease with previous aortic replacement and persistent mitral stenosis
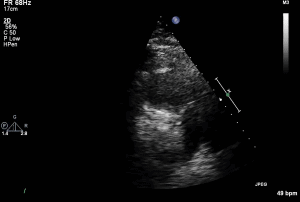
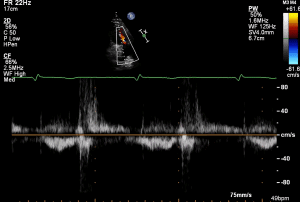
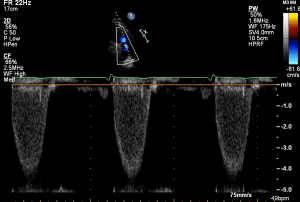
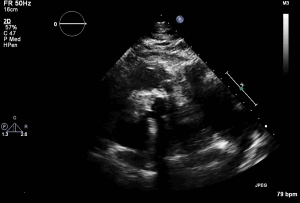
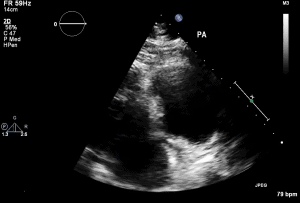
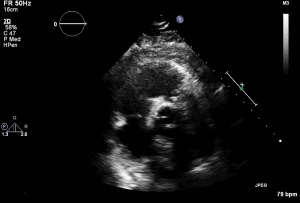
- TTE shown from 2014 but in 2020 progressed to severe and underwent pulmonic replacement
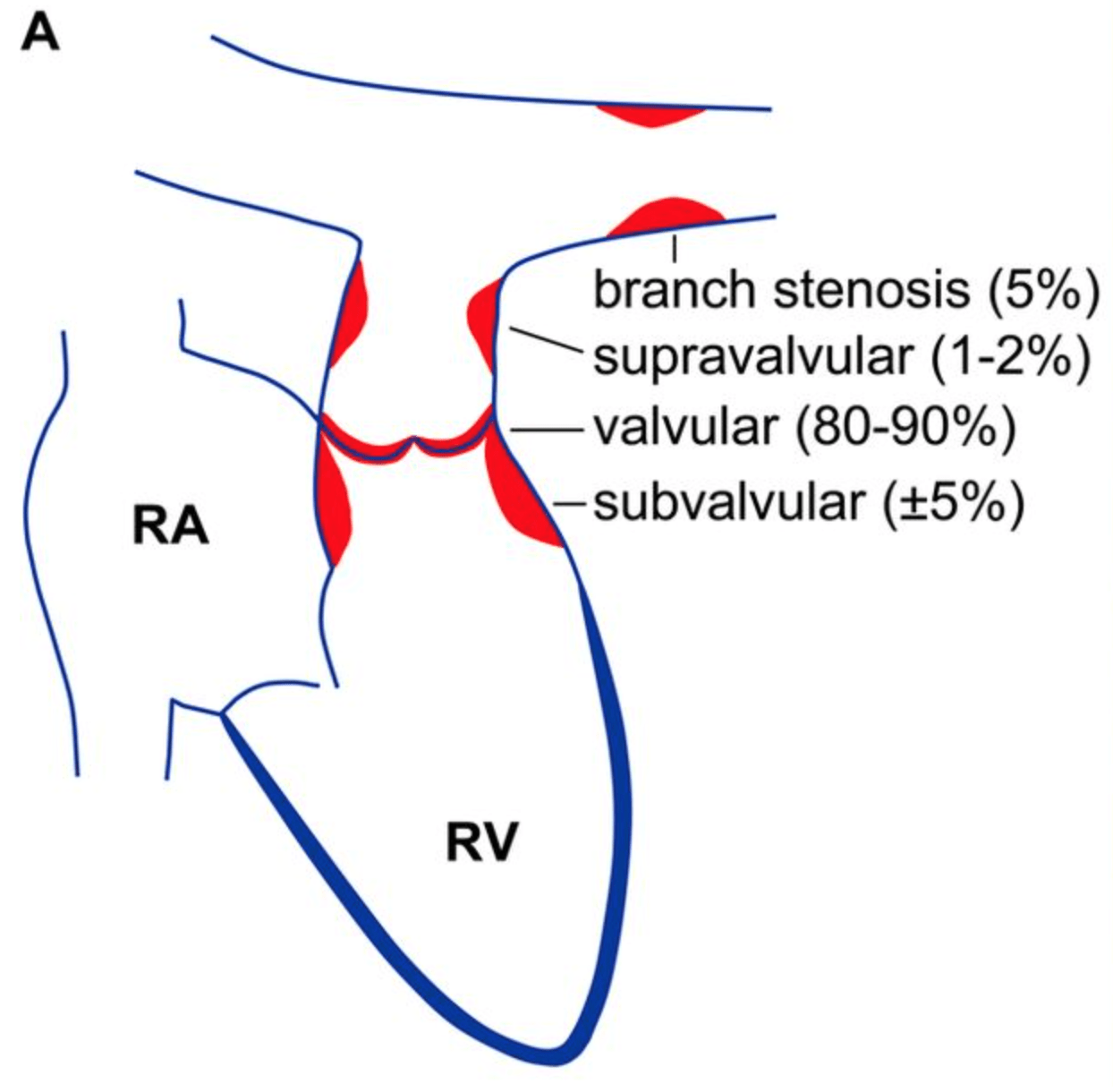
- Moderate PS with max velocity 3.1m/s and mean gradient 39.3 mmHg
- Etiology of PS thought to be congenital
- Mild PR
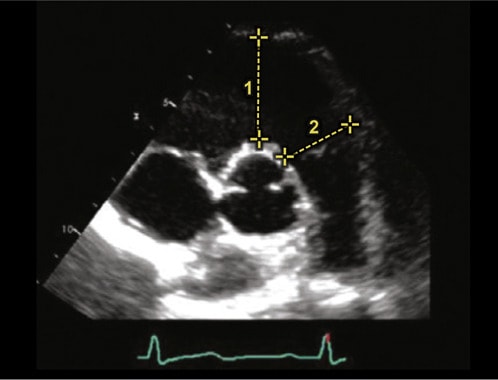
- Severe pulmonary artery dilation