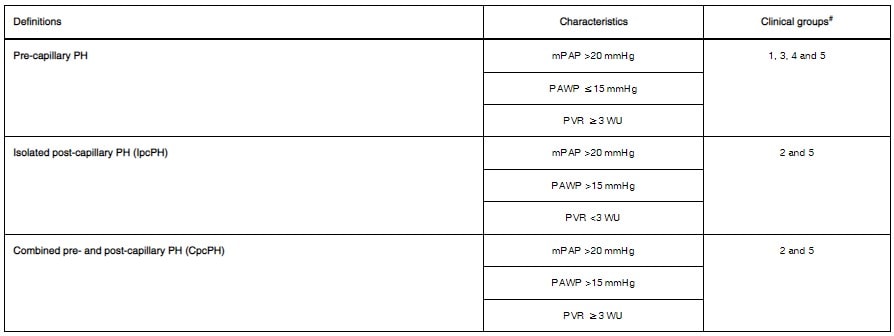
- Pre-capillary vs Post-capillary PH determined based on right heart catheterization
{kind=link}
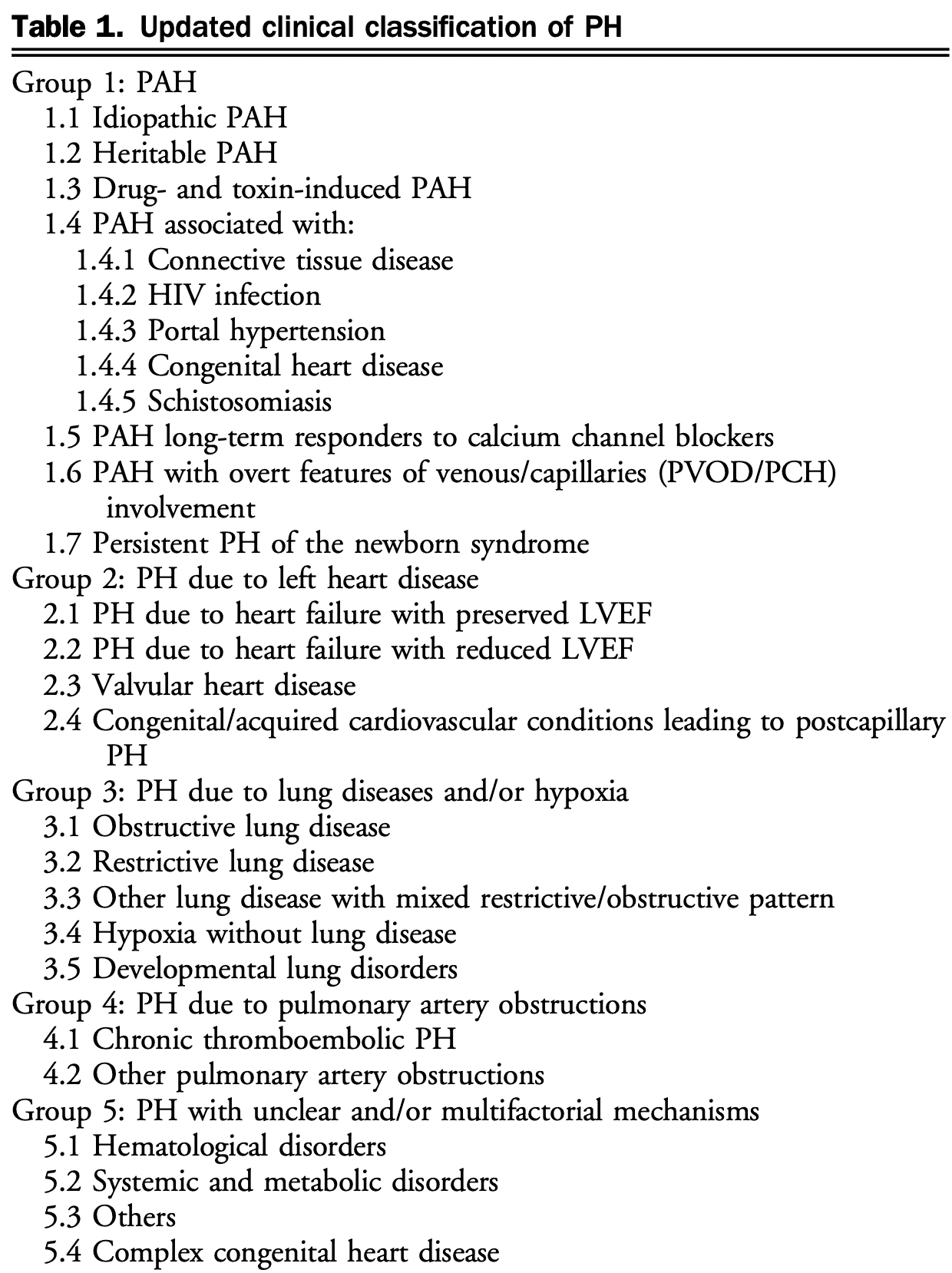
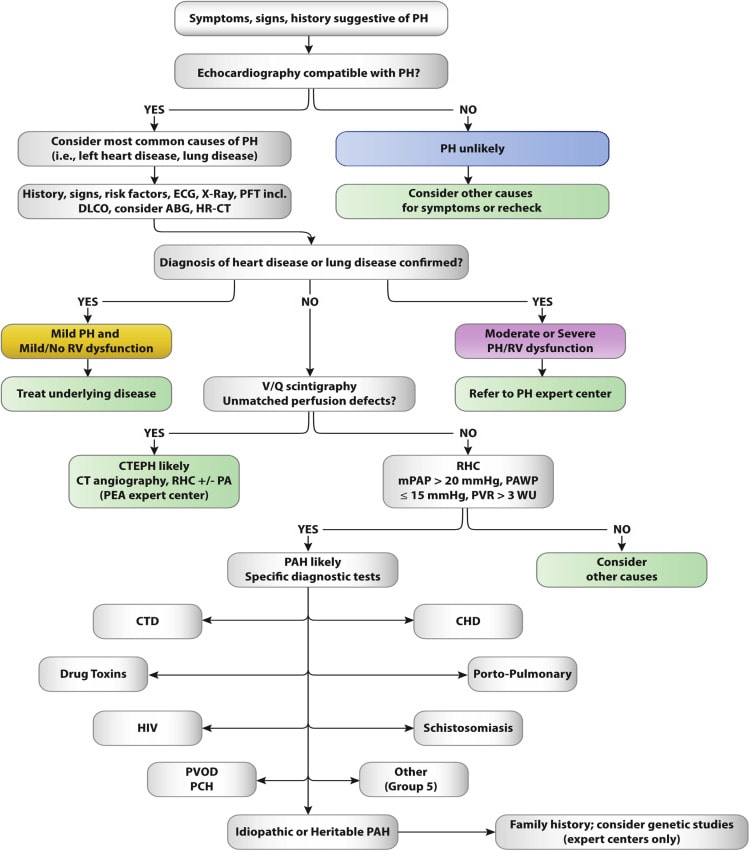
- PAH must be diagnosed by excluding other more common etiologies (left heart disease, lung disease, and CTEPH)
- Vasoreactivity testing in select PAH patients as mentioned above
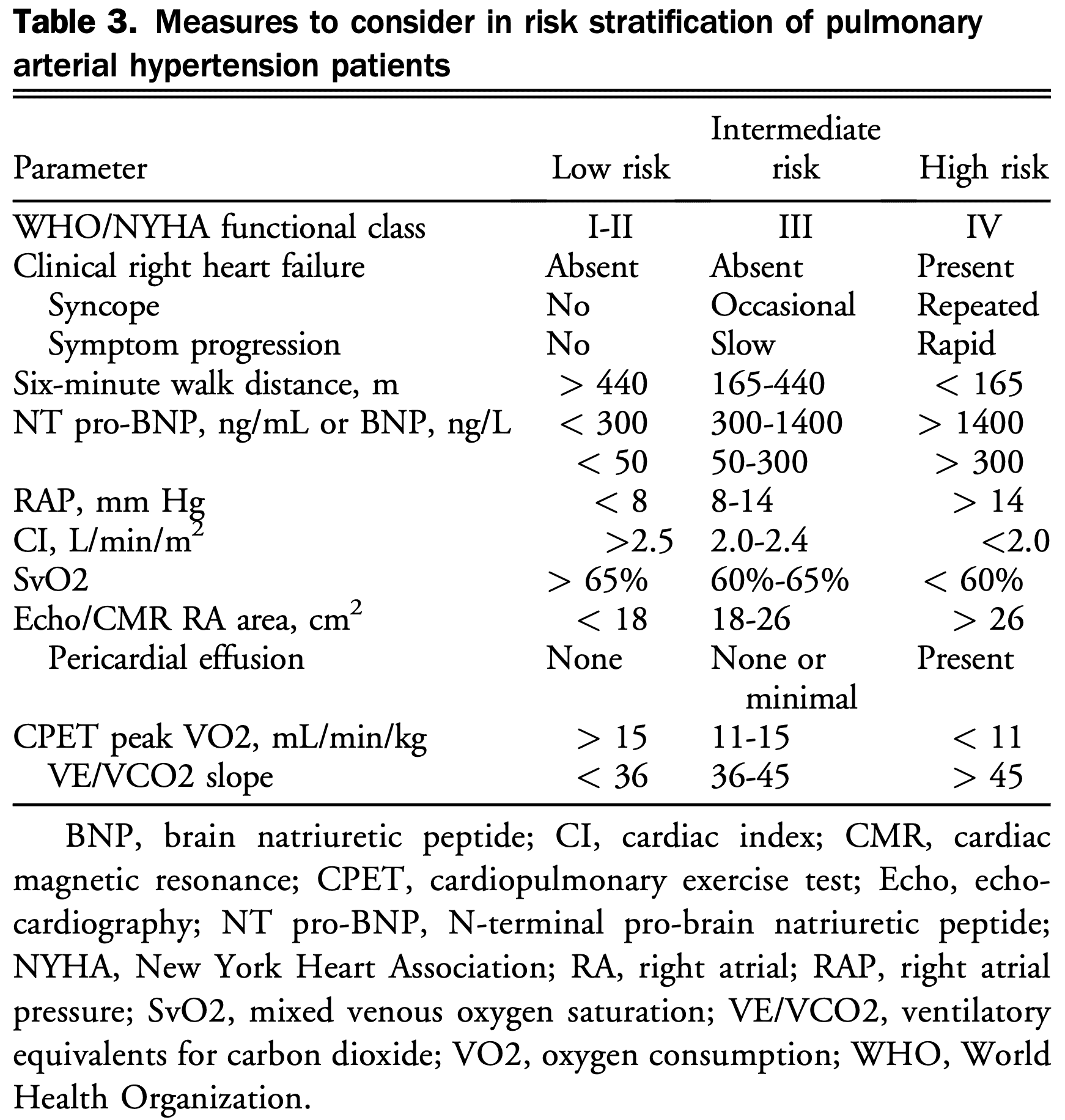
- Risk stratification using a combination of clinical, hemodynamic, and imaging features
{kind=link}