Introduction
- Pericarditis is defined as inflammation of the pericardium.
- 90% of cases are idiopathic or related to viral infections.
- Complications can include:
- Pericardial effusion, tamponade, and constrictive pericarditis.
Etiologies
- Idiopathic: most common, as exact cause is usually not identified
- Infections:
- Viral: Echovirus, Adenovirus, Coxsackievirus, CMV, EBV, Parvovirus, influenza, HIV
- Bacterial: Similar to lung infections, can also be from extension of primary lung infection. Staph, Strep, Pneumococcus, Haemophilus, Mycoplasma, Legionella, Gonococcus
- Fungal: Coccidioidomycosis, Histoplasmosis
- Mycobacterium: Tuberculosis, Avium
- Parasites: Toxoplasmosis, Echinococcosis
- Neoplastic:
- Primary: Angiosarcoma, mesothelioma, paraganglioma, lipoma
- Secondary: Lung, breast, lymphoma, GI, melanoma, Kaposi sarcoma
- Inflammatory:
- Myocarditis
- Collagen diseases: Lupus, rheumatoid arthritis, scleroderma, Sjogren’s syndrome
- Vasculitis: Giant cell arteritis, Churg-Strauss syndrome, polyarteritis nodosa
- Rheumatic fever
- Inflammatory bowel disease
- Sarcoidosis
- Medications: Hydralazine, procainamide, doxorubicin, cyclosporine, cyclophosphamide
- Radiation
- Trauma
- Post-myocardial infarction
- Congenital: absence of pericardium
- Renal failure (uremic)
Diagnosis
Clinical Presentation
- Pleuritic retrosternal chest pain
- Pain often radiates to back or trapezius
- Pain is worse when lying flat and relieved by sitting forward
- Associated symptoms: dyspnea, fever, tachycardia, and occasionally signs of tamponade
- Pericardial friction rub is a “classic/pathognomonic” finding, best heard with the patient sitting forward on end expiration
Diagnosis confirmed if 2 out of 4 classic features
- 1) Classic pleuritic chest pain that is positional
- 2) Typical ECG changes
- 3) Pericardial friction rub
- 4) Pericardial effusion
{kind=link}
Investigations
- Standard bloodwork: CBC, lytes, urea, creatinine, liver enzymes
- Troponin – if positive, consider myopericarditis or prior myocardial infarction.
- CRP – confirm inflammatory process; most patients with pericarditis will have an elevated CRP. Therefore, helpful test to rule out pericarditis if negative. Also useful for tracking response to treatment.
- ECG – look for classic features of pericarditis or alternate condition as cause of chest pain, i.e. STEMI.
- Chest X-ray – look for enlarged cardiac silhouette to suggest pericardial effusion.
- Echocardiogram – look for pericardial effusion and assess heart function.
- Depending on clinical suspicion, consider any of: autoimmune work-up (ANA, ANCA, RF), HIV, HCV, TSH, malignancy work-up.
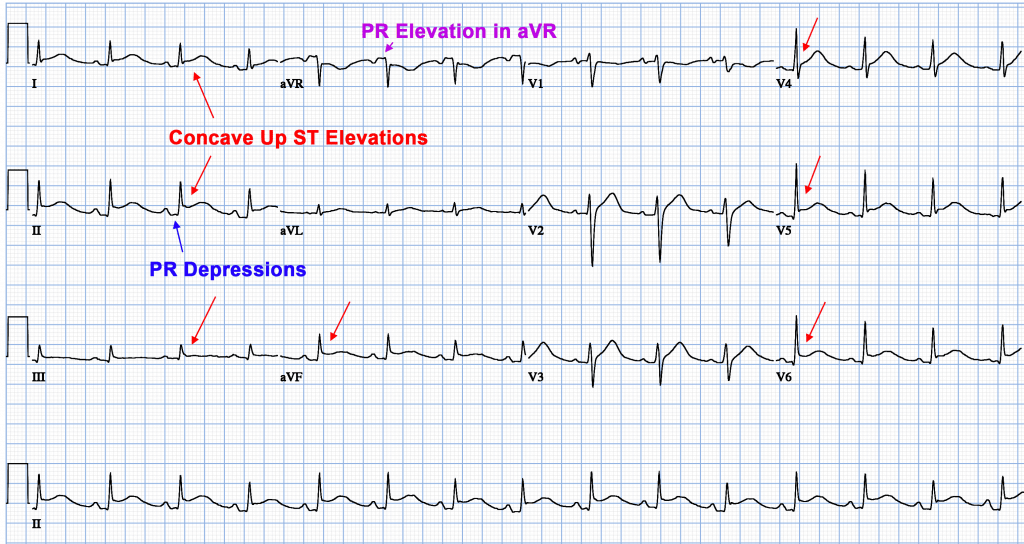
ECG (4 Phases)
- Diffuse ST elevation (upsloping/concave), with PR depression, and reciprocal changes in aVR
- Normalization of ST segments
- T-wave inversions
- T-wave normalization
Echo
- Look for pericardial effusion, as most patients will have this in pericarditis.
- Must rule out cardiac tamponade clinically (echocardiogram can be helpful).
- Pericardiocentesis is rarely required unless there is tamponade physiology, or suspected bacterial or malignant cause.
{kind=link}
{kind=link}
{kind=link}
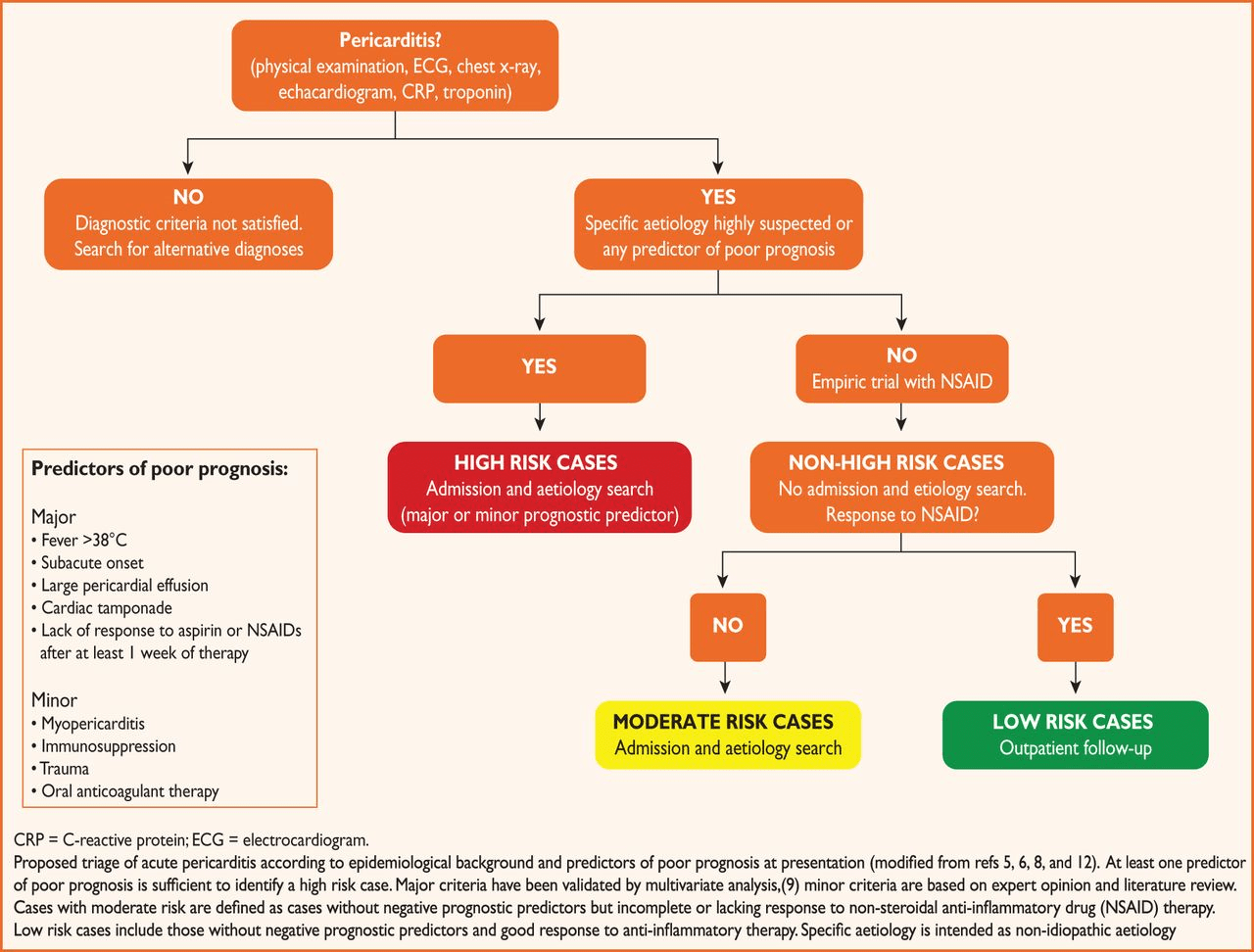
Patient Triage
- If any predictors of poor prognosis are present (below) or if no response to NSAIDS, patient should be admitted and etiology investigated.
(clinicians should be well familiar with the factors below)- Major predictors of poor prognosis
- Fever > 38°C
- Subacute onset
- Large pericardial effusion
- Cardiac tamponade
- Lack of response to NSAID after 1 week of therapy
- Minor predictors of poor prognosis
- Myopericarditis
- Immunosuppression
- Trauma
- Oral anticoagulant use
- Major predictors of poor prognosis
- Consider POCUS to assess for large effusion before discharge.
{kind=link}
Treatment
- High dose NSAIDs (i.e. Ibuprofen 600-800 mg QID) or ASA (650 mg QID) for 1-2 weeks.
- Colchicine 0.5 mg bid or if body weight is less than 70 kg, colchicine 0.5 mg daily for 3 months (decreases recurrence).
- Low dose corticosteroids (ie. 0.2-0.5mg/kg/day) can be used in patients with failure/contraindication to ASA/NSAIDS with colchicine or with autoimmune etiology.
- The downside of corticosteroids is a risk of recurrent pericarditis. Often patients with pericarditis on corticosteroids must remain on them for up to 6 months with a very slow taper (see ESC 2015 guideline for taper recommendations)
- Proton pump inhibitor while on high dose NSAIDs/ASA.
- Patients on dialysis with suspected uremic pericarditis, may benefit form intensified dialysis.
"Myopericarditis" and "Perimyocarditis"
- Commonly the causes of pericarditis can contribute to direct myocardial injury resulting in damage and elevation of cardiac biomarkers (troponin and CK-MB).
- “Myopericarditis” and “perimyocarditis” are often incorrectly used interchangeably.
- Myopericarditis implies a primary pericardial issue with elevated cardiac biomarkers but normal left ventricular function. Pain can be treated similarly to in acute pericarditis but some authors have argued reduced NSAID dose. (Animal models have suggested increase myocardial inflammation and increase in mortality.) No strong evidence for colchicine.
- Perimyocarditis implies a primary myocardial issue with elevated biomarkers AND left ventricular dysfunction with regional wall abnormalities. Generally avoid NSAIDs in patient with reduced heart function as they can worsen heart failure, increase hospitalization, and increase mortality.
Exercise Restrictions
- Pericarditis (non-athlete) – restrict exercise until resolution of symptoms and normalization of CRP, ECG, and echocardiogram.
- Pericarditis (athlete) – restrict exercise until resolution of symptoms and normalization of CRP, ECG, and echocardiogram, and for a minimum of 3 months.
- Myocardial involvement – restrict exercise for a minimum of 6 months for both athletes and non-athletes because of the small risk of sudden cardiac death.
Further Reading
- 2015 ESC Guidelines for the Diagnosis and Management of Pericardial Diseases (html) (pdf)
- Pericardial Disease. William C. Little and Gregory L. Freeman. Circulation. 2006;113:1622–1632
- Primary Author: Dr. Daniel Durocher (MD, FRCPC, Cardiology Fellow)
- Author/Reviewer: Dr. Atul Jaidka (MD, FRCPC, Cardiology Fellow), Dr. Pavel Antiperovitch (MD, FRCPC)
- Staff Reviewer: Pending
- Copy Editor: Perri Deacon (medical student)
- Last Updated: May 31, 2020