Though rheumatic mitral stenosis is the most common cause of mitral stenosis, calcific mitral stenosis is becoming more common in elderly populations
In contrast to rheumatic, calcification starts at the base and usually spares the leaflet tips
No commissural fusion
Determination of severity is difficult as planimetry is challenging
Interventions
No role for PMBC or surgical commissurotomy
Surgery is technically challenging as mitral annular calcification causes difficulty in securing a prosthesis
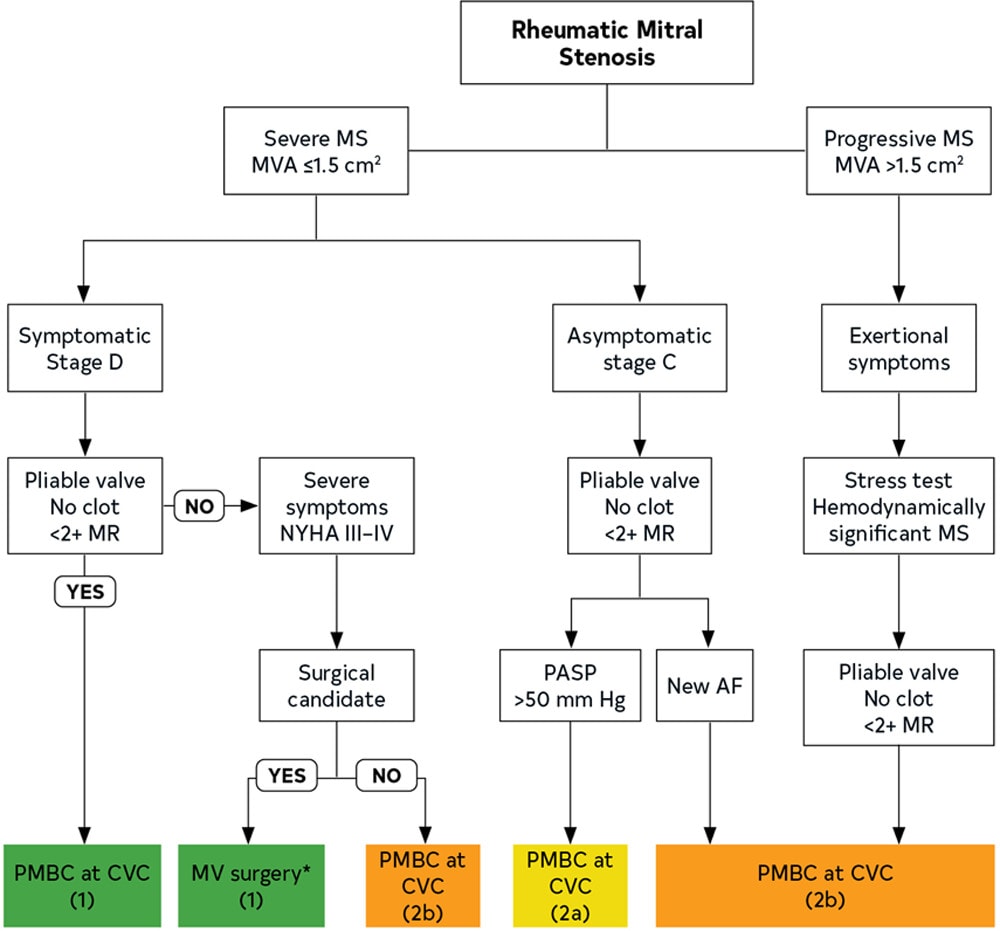
Guidelines recommend valve intervention in patients with severe symptoms (NYHA III or IV), severe mitral stenosis (mitral valve area < 1.5 cm2) and after discussion of the high operative risk with the patient
Further Reading
2020 AHA: Guideline for the Management of Patients With Valvular Heart Disease (html) (pdf)