Echocardiography plays a central role in the field of cardio-oncology
Many of the trials use LVEF in the definition for cardio-toxicity
Ongoing area of research to determine how early and how best to predict cardiac complications of cancer therapy
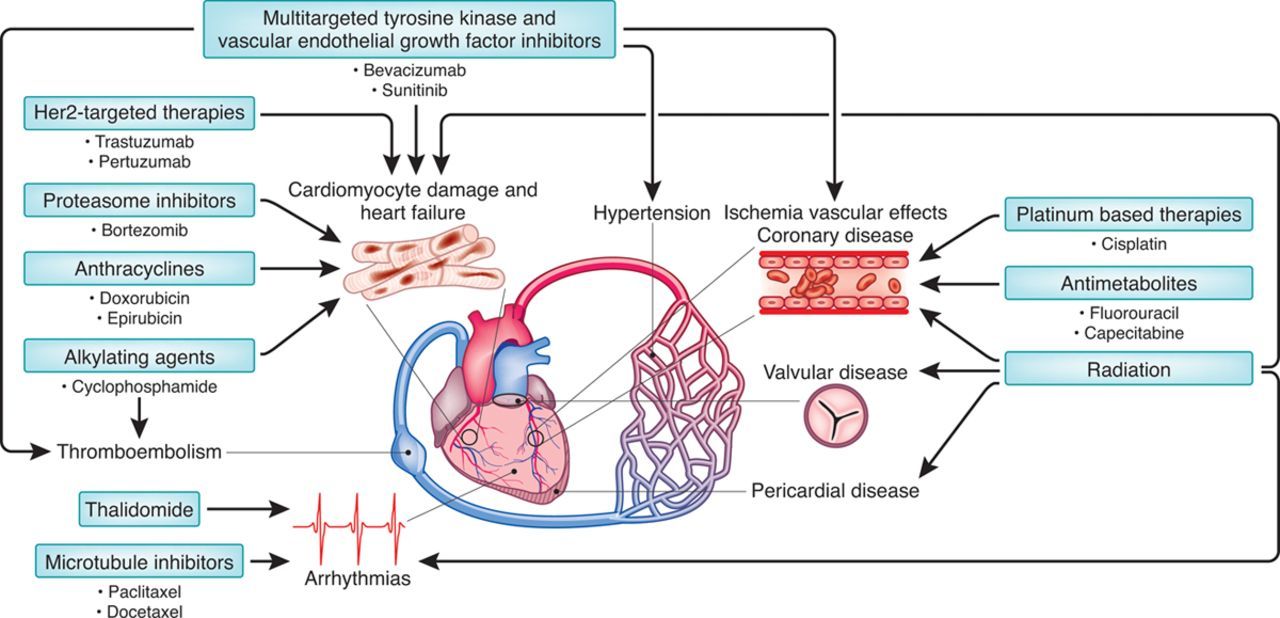
Cardiac Complications of Chemotherapy and Radiation
Cardiomyopathies
LV dysfunction (HFpEF or HFrEF)
Myocarditis
Takotsubo
Thrombus
Infiltration
Vascular Disease
Arterial stiffness
Accelerated athersclerosis
Pericardial Disease
Tamponade
Constriction
Pulmonary Hypertension
RV Dysfunction
Valvular Disease
Regurgitation
Stenosis
Endocarditis
Arrhythmias
QTC prolongation
Circ Res 2016: An overview of the cardiovascular side effects of chemotherapy and radiation
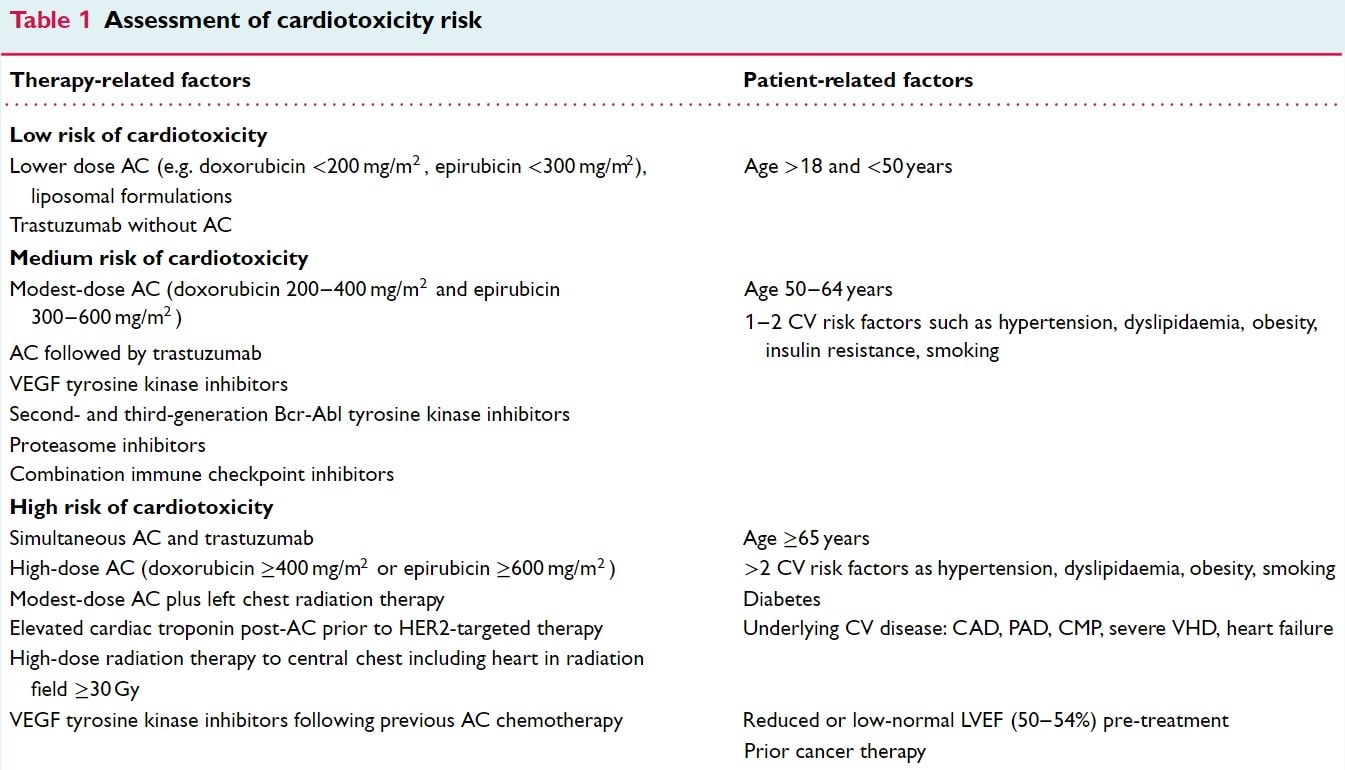
ESC 2020: Assessment of Cardiotoxicity Risk
Frequency of Monitoring
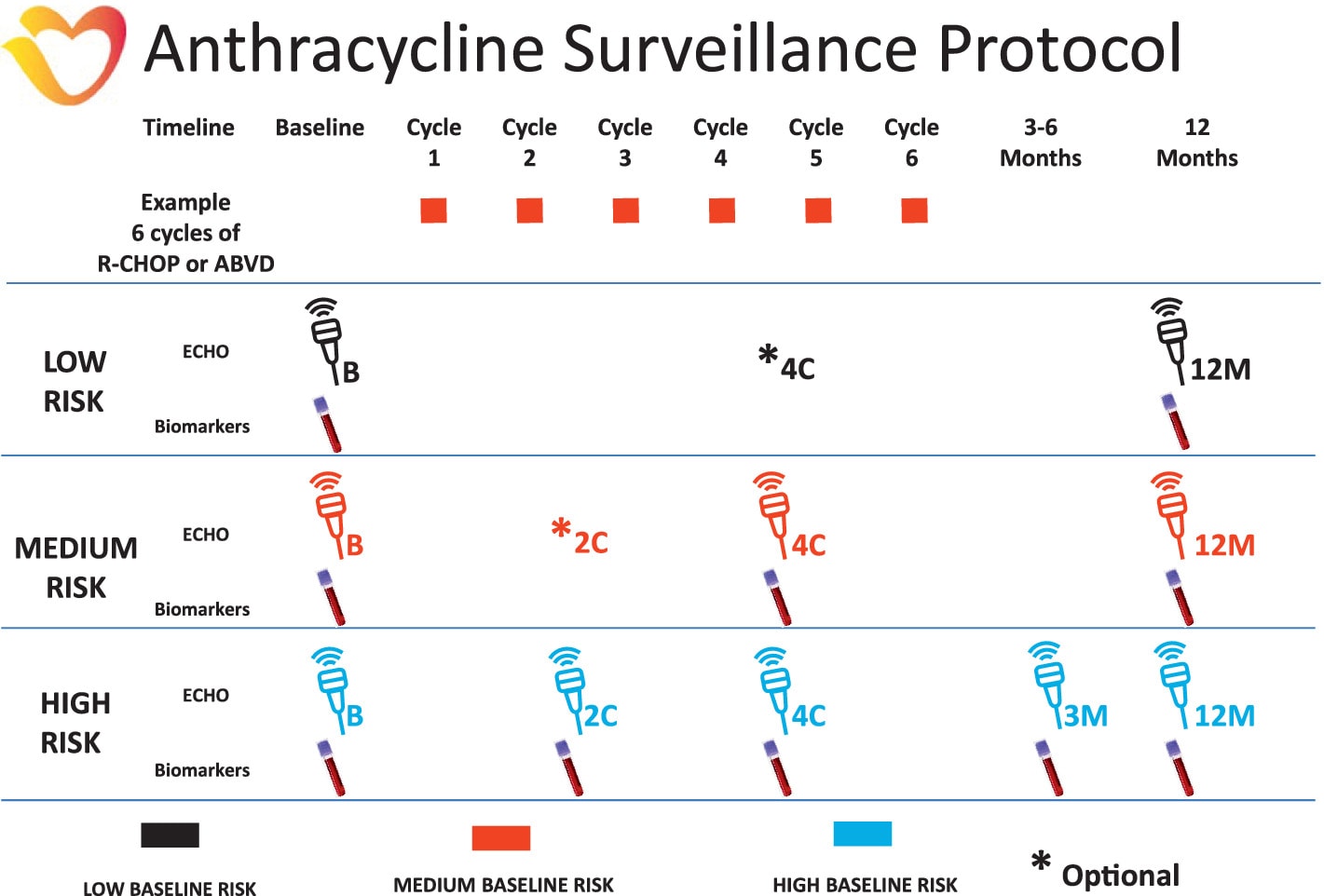
Surveillance is initially stratified by baseline risk (low, medium, high) and then frequency is determined by chemotherapy cycles while on treatment and monthly after treatment
Recommendations vary greatly between guidelines
CCS does not have any recommendation for anthracyclines and recommends q3months for Anti-HER2
Example surveillance protocols below from ESC
Example Anthracycline Surveillance Protocol from ESC
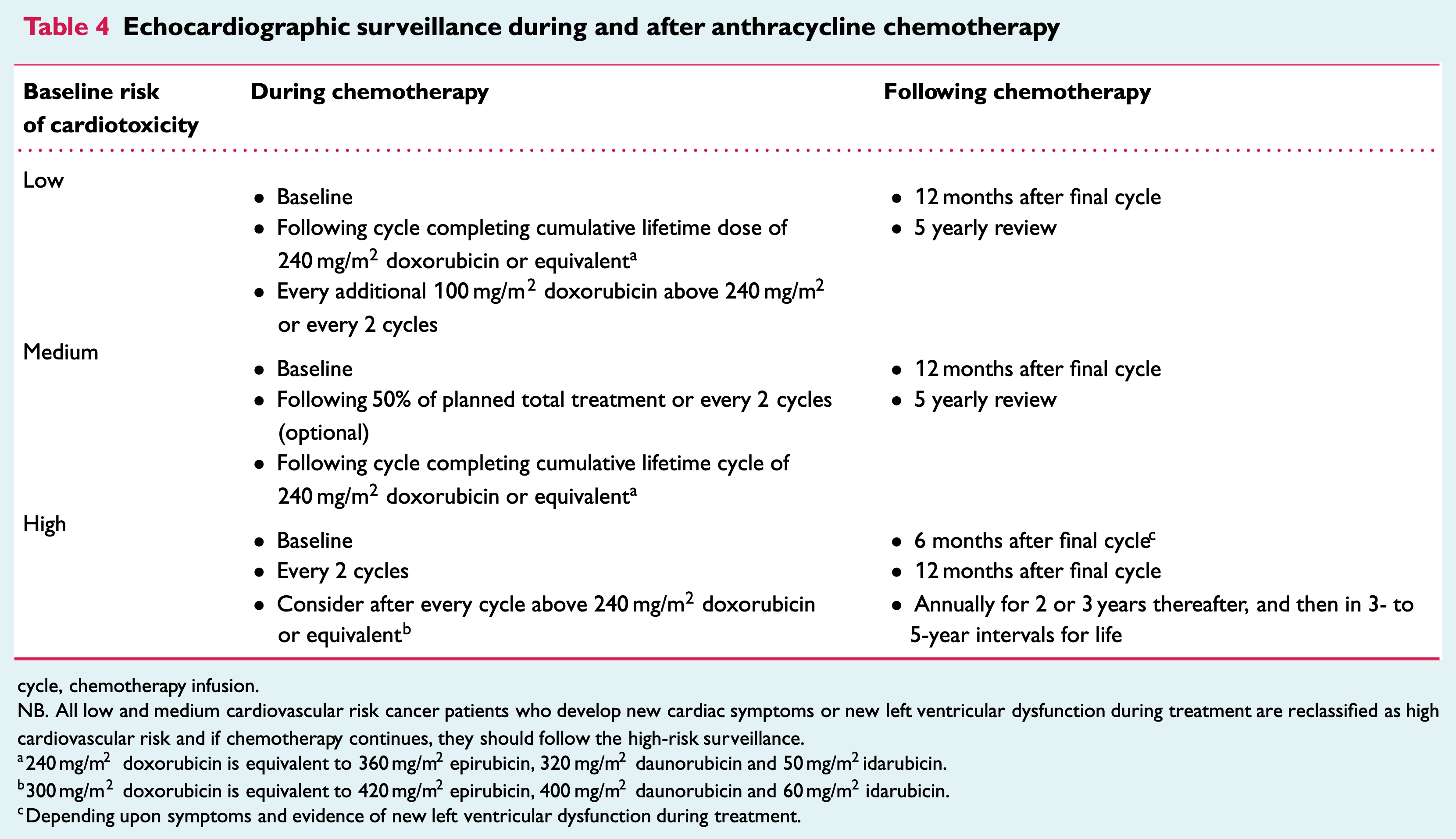
ESC 2020: Echocardiographic surveillance during and after anthracycline chemotherapy
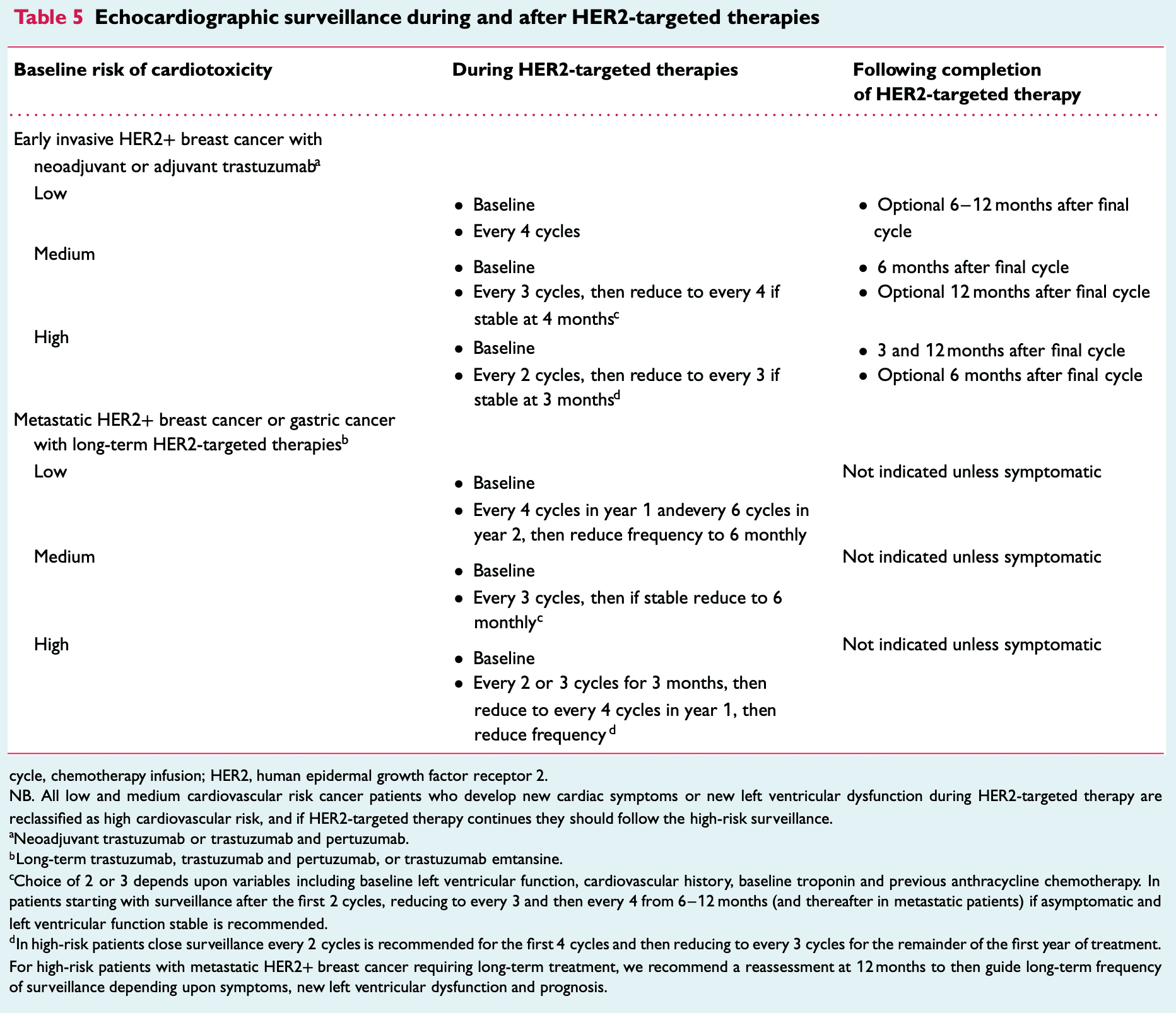
ESC 2020: Echocardiographic surveillance during and after HER2-targeted therapies
BSE 2021: Frequency of Echo Monitoring During Anthracycline or Anti-HER2
Echo Assessment
Definition of Cancer Treatment Related Cardiac Dysfunction (CRTCD)
EF drop of >10% from baseline and <50% (or 50%)
Relative reduction in GLS > 15% from baseline
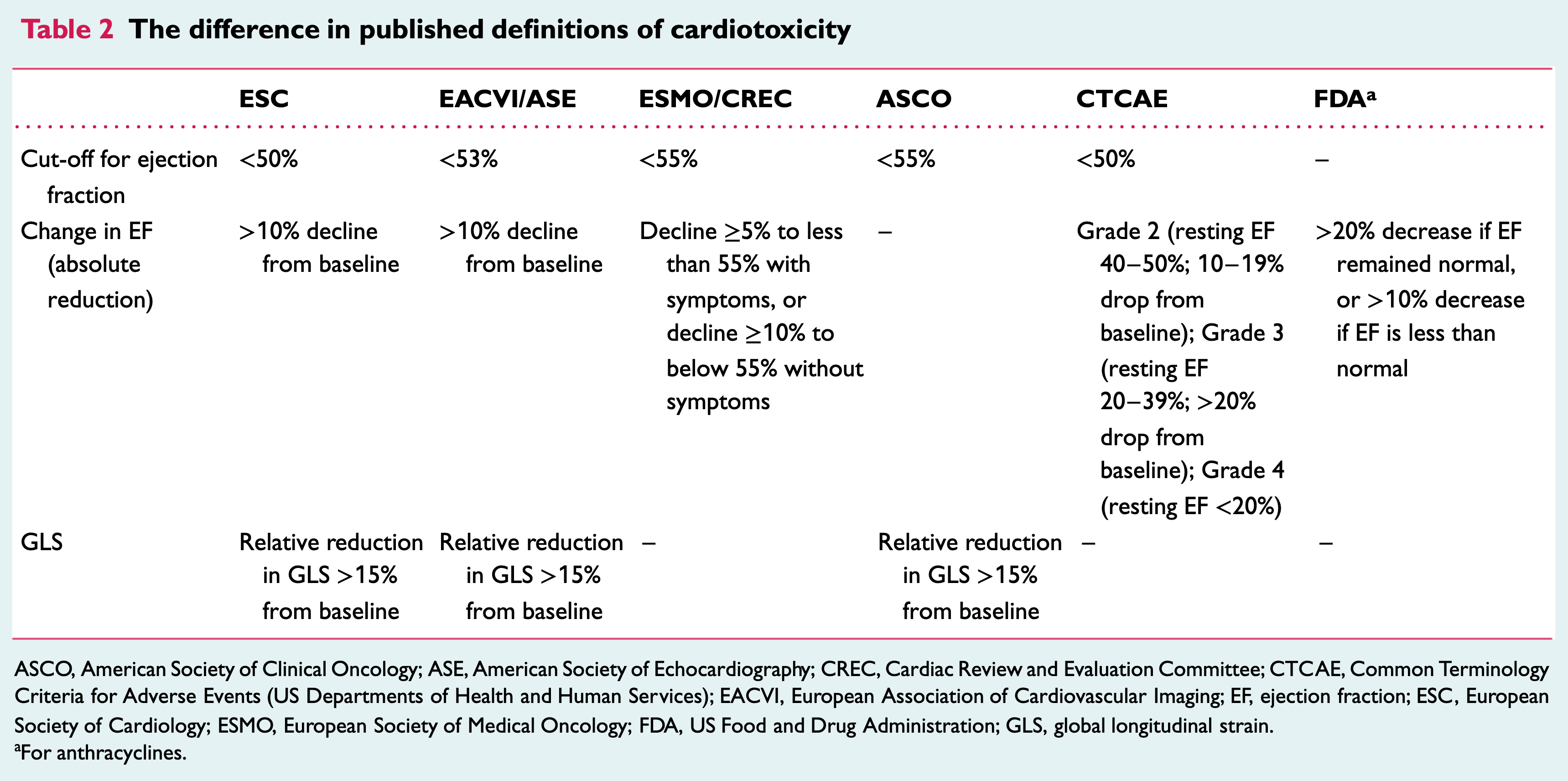
ESC 2020: The difference in published defnitions of cardiotoxicity
Echo Protocol
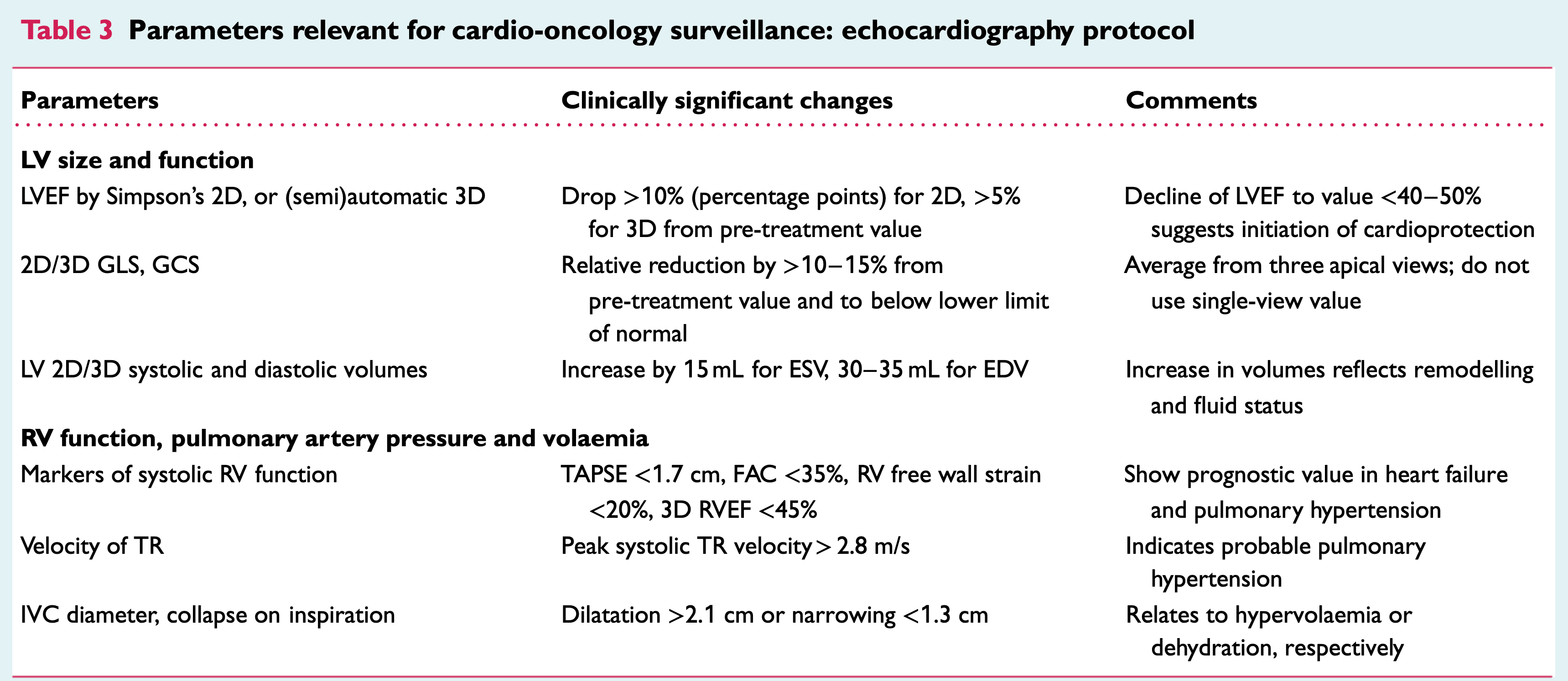
ESC 2020: Parameters relevant for cardio-oncology surveillance: echocardiography protocol
LV Systolic Function
2D EF
Acquisition
Images should be acquired at end-respiration
Simpsons method preferred
In atrial fibrillation use beats with similar R-R interval
3D EF
Acquisition:
High-quality ECG with clear R-wave (used for software to trigger full volume)
Recommend breath hold with shallow breathing, preferably end-expiration (if deep inspiration needed, recommended to document and recreate at next exam)
Review images before patient patient leaves to look for stitch artifact and ensure if contouring possible
Some variations between software thus should use same machine and analysis software for serial echo
Sensitive to image quality thus 2D and 3D images should be taken
Benefits:
No assumptions made about LV geometry (ie. short axis view of ventricle is circular)
Ability to discriminate smaller % changes (5-8%)
Semi-automated and thus better intra- and interobserver variability
Contrast
Poor endocardial definition can occur in patients post mastectomy, chest radiation or breast reconstruction surgery)
Contrast should be used when 2 contiguous LV segments from any apical view are no adequately visualized
LV Diastolic Function
Diastolic dysfunction may appear earlier than systolic dysfunction so important to acquire on each exam
Global Longitudinal Strain
Acquisition:
GLS is calculated using A3C/A4c/A2c views with optimal image quality and frame rate 40-90
If more than 2 segments have poor tracking, GLS should not be calculated
Some variations between software thus should use same machine and analysis software for serial echo
ASE 2015: “peak GLS in the range of -20% can be expected in a healthy person, and the lower the absolute value of strain is below this value, the more likely it is to be abnormal”
Cardiotoxicity defined as relative reduction in GLS > 15% from baseline
Currently being studied how well GLS can predict cardiotoxicity (SUCCOUR study + commentary)
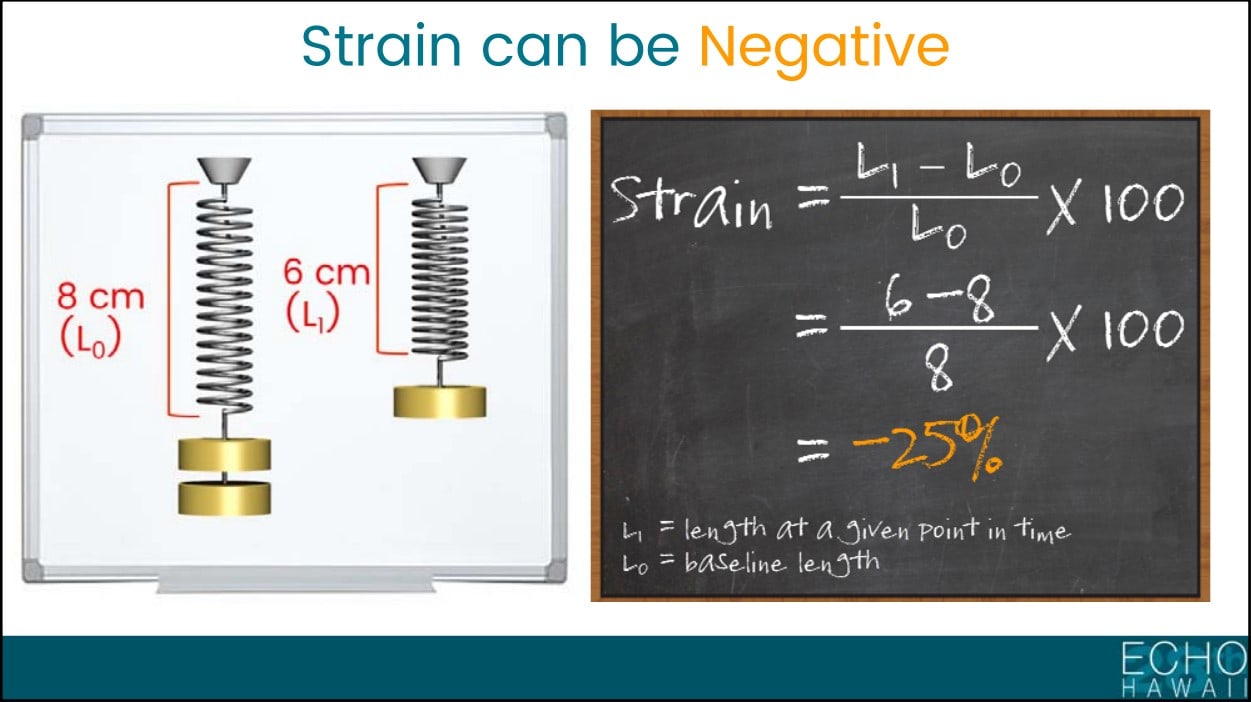
Beginner’s Guide to Strain - Bonita Anderson
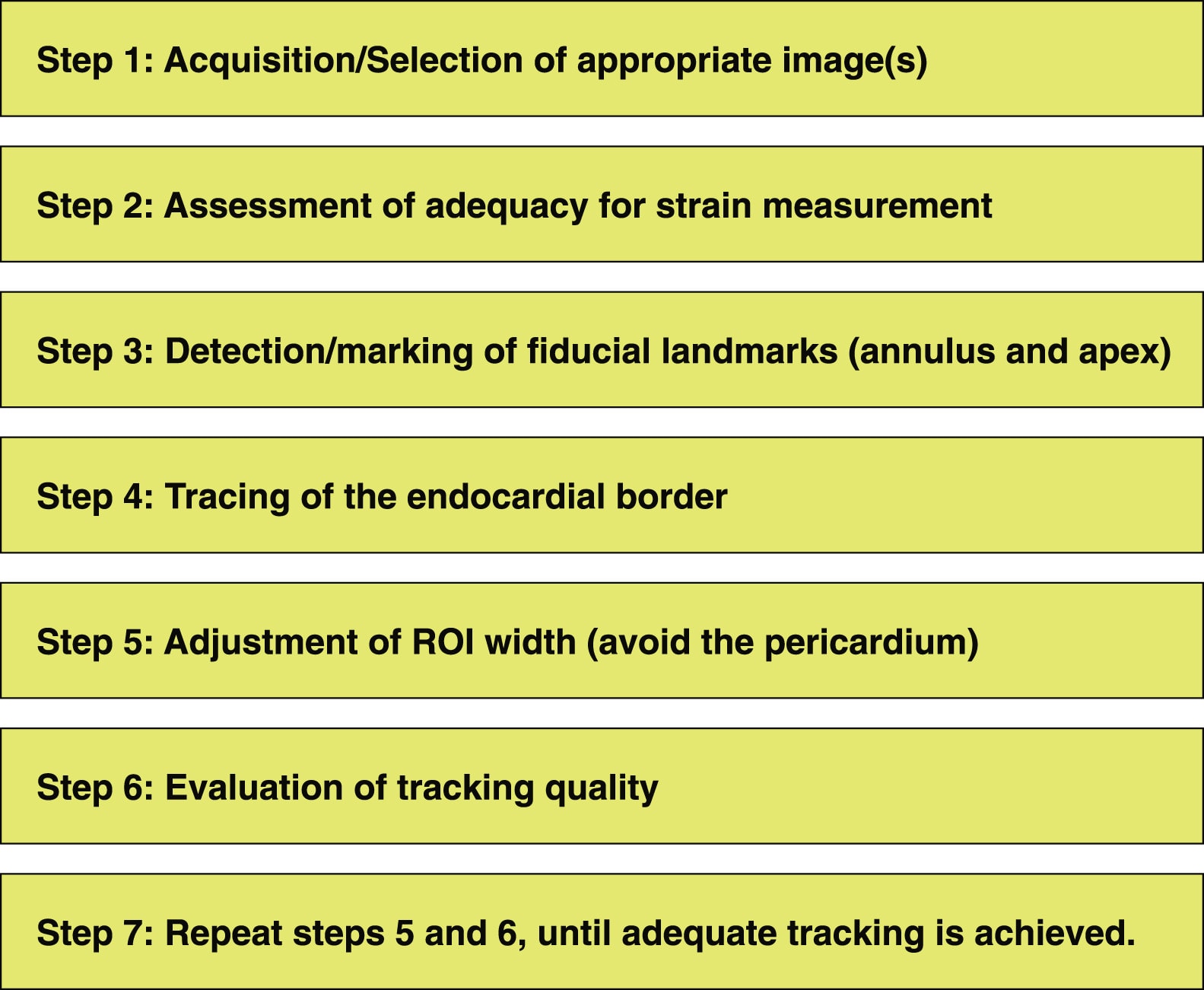
JACC 2015: Steps for Myocardial Strain Measurement
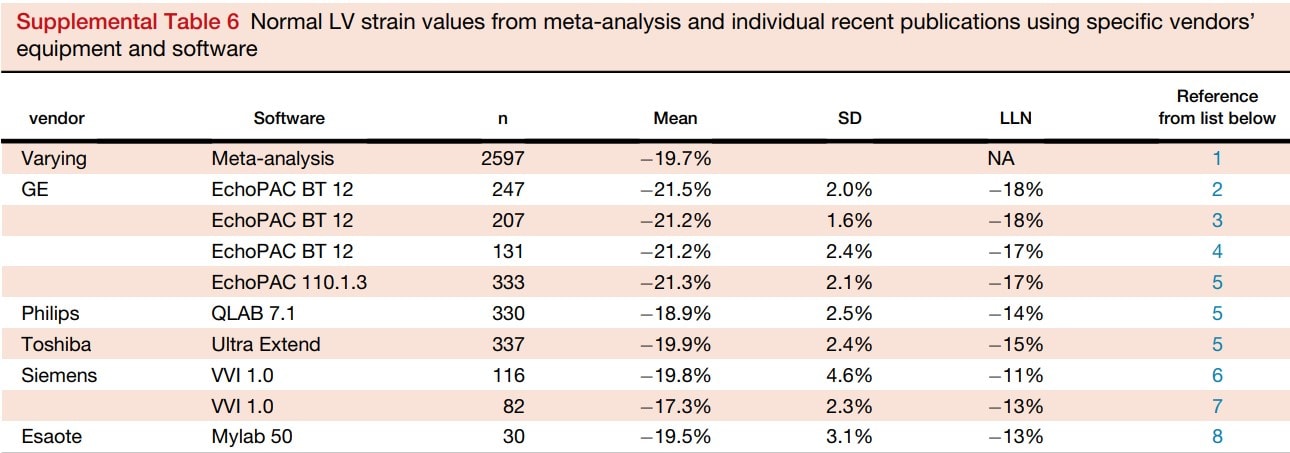
ASE 2015:Normal LV strain values from meta-analysis and individual recent publications using specific vendors’
Right Heart
Not officially included in the definition of cancer treatment related cardiac dysfunction
Recommended parameters as expected: RV dimenions, RV S’, TAPSE, TR Velocity, FAC
Certain cancer treatments can cause PH (dasatinib) and/or RV dysfunction (anthracycline, anti-HER2, cyclophosphamide, dasatinib)
Radiation Related Cardiac Dysfunction
Pericardial disease is the most frequent radiation related complication
Can occur months to years later
Should assess for constriction and pericardial effusion
Valvular disease can occur with radiation
Fibrotic process which can cause leaflet thickening, shortening and calcifications that may result in stenosis or regurgitation
More often left-sided valves
Recommended to image 5 years after RT in high risk patients and 10 years in non high risk followed by q5years
Multimodal Imaging
CT
Useful in non-invasive evaluation of coronary disease, pericardial disease, and cardiac tumours
MRI
Useful in patients with poor echocardiographic windows
Great inter- intrareader variability and thus sensitive in detecting small changes in EF
Tutorials
Phillips EPIQ Strain Tutorial
Phillips Dynamic Heart Model (Single-Beat) Tutorial
Case
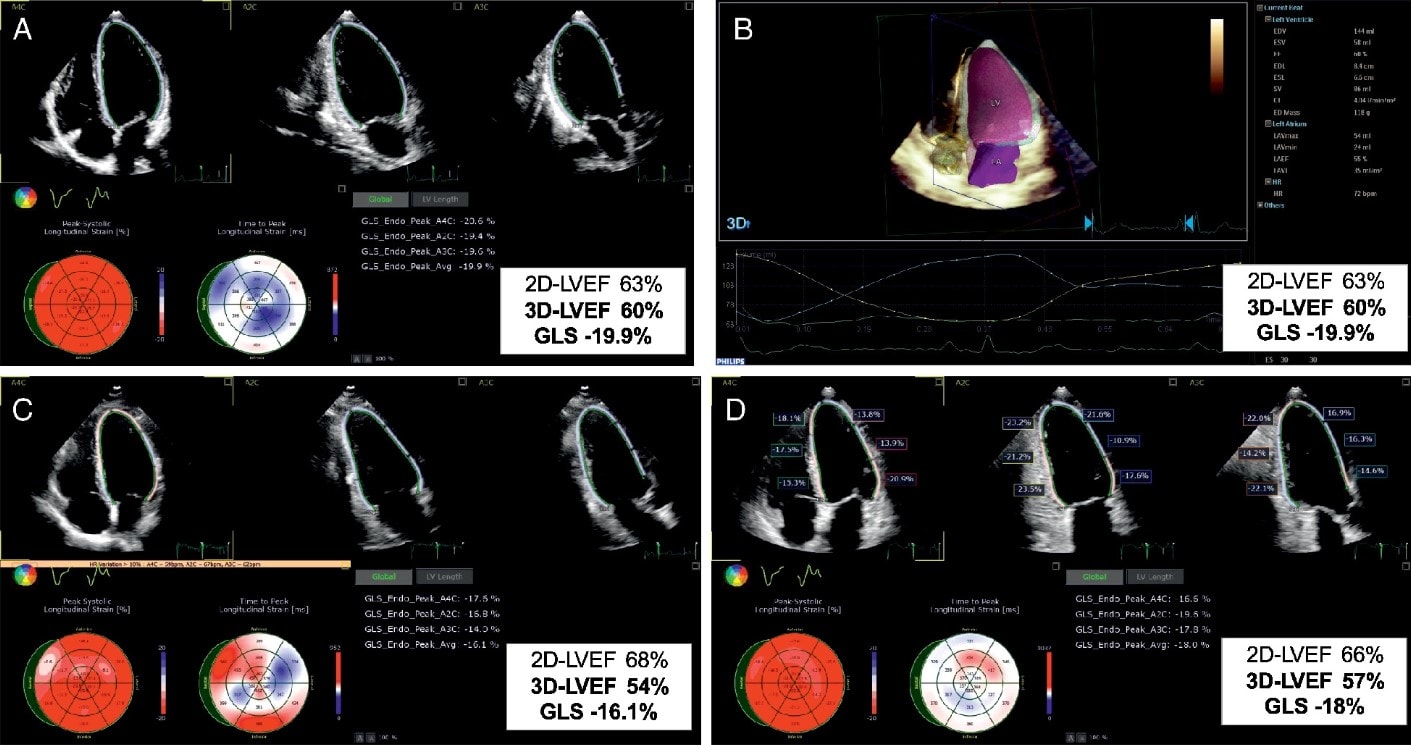
The case of a 66‐year‐old female with invasive breast ductal carcinoma (ER+ HER2+) treated by the combination of doxorubicin, cyclophosphamide, paclitaxel, radiotherapy (35 Gy + 10) and trastuzumab. (A) Baseline apical two‐dimensional (2D) echocardiographic four‐, two‐ and three‐chamber views, showing normal left ventricular ejection fraction (LVEF), with speckle tracking‐derived bull's eye and normal global longitudinal strain (GLS). (B) Baseline three‐dimensional (3D) volumetric analysis of the left ventricle and left atrium; measurements are normal. (C) At 3‐month follow‐up, 2D LVEF remains normal, while 3D LVEF drops by 10% and GLS by 19%. This entailed the initiation of anti‐remodelling treatment with no interruption of oncologic drugs. (D) At 6‐month follow‐up, while continuing cancer and cardiac medications, the 3D LVEF reversed by 5%, and GLS recovered by 10%.
Further Reading
2020 HFA/EACVI/ESC: Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies (html) (pdf)
2021 BSE/BCOS: Guideline for Transthoracic Echocardiographic Assessment of Adult Cancer Patients Receiving Anthracyclines and/or Trastuzumab (html) (pdf)
2015 ASE/EACVI: Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults (html) (pdf)
2015 JACC: Practical Guidance in Echocardiographic Assessment of Global Longitudinal Strain (html) (pdf)