Atrial rhythm ≥ 100bpm initiated from a discrete origin
Ventricular rate varies depending on AV nodal conduction
Can be paroxysmal, sustained, or incessant
ECG Features
The key is to find the P-waves!
Depending on velocity of AV conduction, P-waves can be located anywhere in the cycle (commonly in the QRS or T-wave)
P-waves often have different morphology to sinus P-waves (compare to sinus ECG)
Caveat: P-wave morphology can match sinus P-waves when the focus is close to the sinus node.
P-wave morphology can resemble retro-conducted P-waves if the origin is low in the atrium or close to the AV node.
Sometimes a “Warm-Up” and “Cool-Off” phenomenon can be seen where the tachycardia accelerates and gradually slows down before terminating.
SVT that terminates on a P-wave is significantly less likely to be AT
Explanation: If a tachycardia terminates on a P-wave, the atrial focus must stop firing, and the AV node must block on the same beat. Both of these events are statistically unlikely to happen on the same beat.
Sinus Tachycardia: Note that there is a discrete initiation with an early P-wave. Termination happens on a QRS.
Unlikely to be sinus tachycardia: Terminates on a P-wave
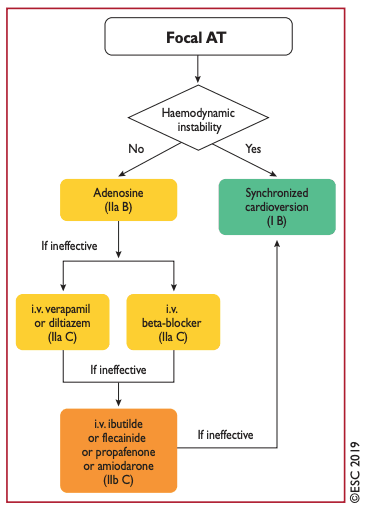
Response To Adenosine
Adenosine blocks the AV node, which stops ventricular activation, revealing AT P-waves.
Compare these P-waves to the sinus ECG.
Usually P-waves are discrete and separated by an isoeletric period
Tachycardia continues after adenosine effect wears off.
NOTE: Some atrial tachycardias are adenosine-sensitive, and can slow down or terminate with adenosine.
Localizing Atrial Origin (Advanced)
Negative P wave in lead I and aVL suggests LA origin