Atrial fibrillation is a common supraventricular tachycardia
Incidence in Canada is up to 4.5% per year, with lifetime risk estimated at 25% among those older than 40 years of age
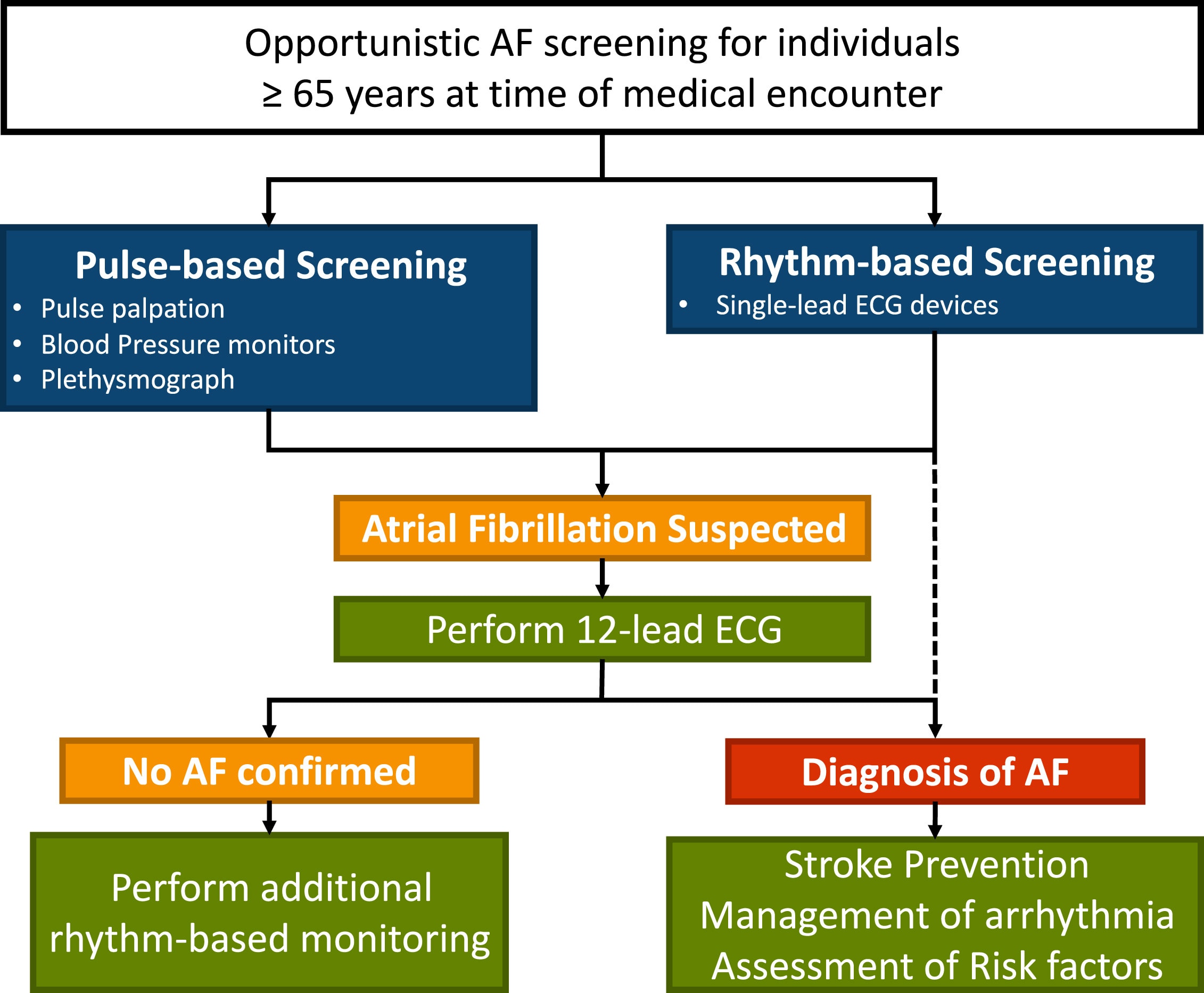
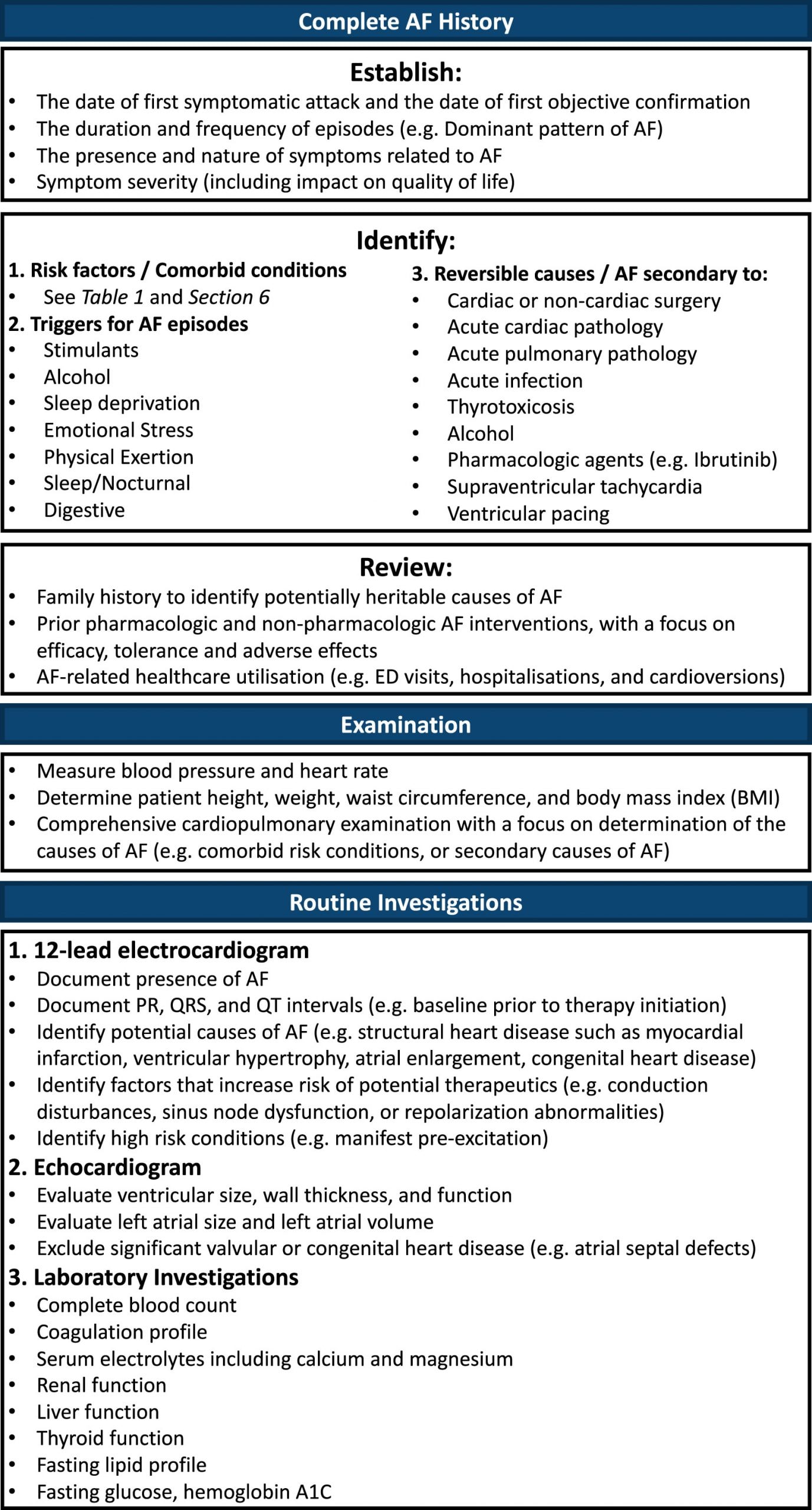
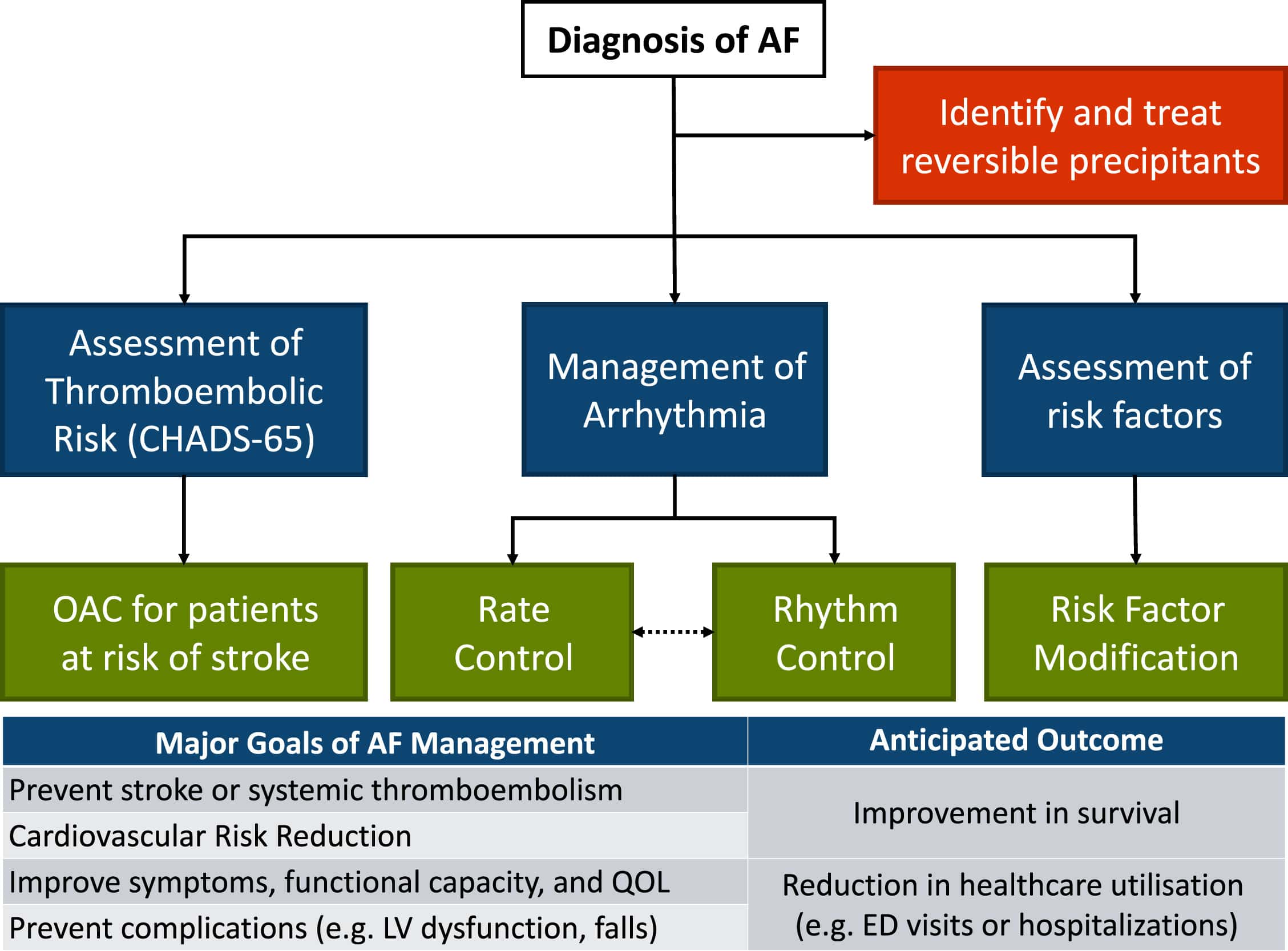
Evaluation of the patient involves:
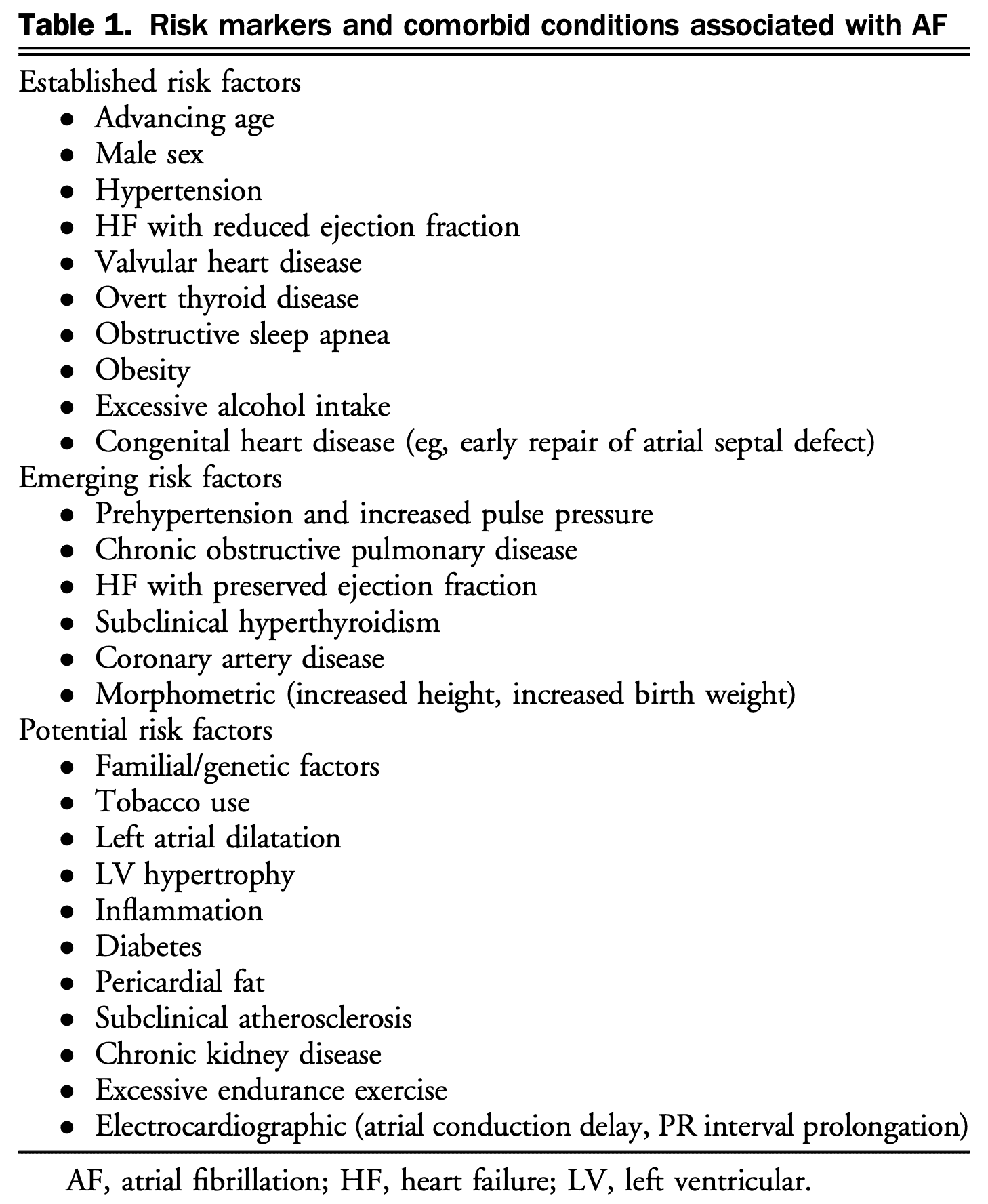
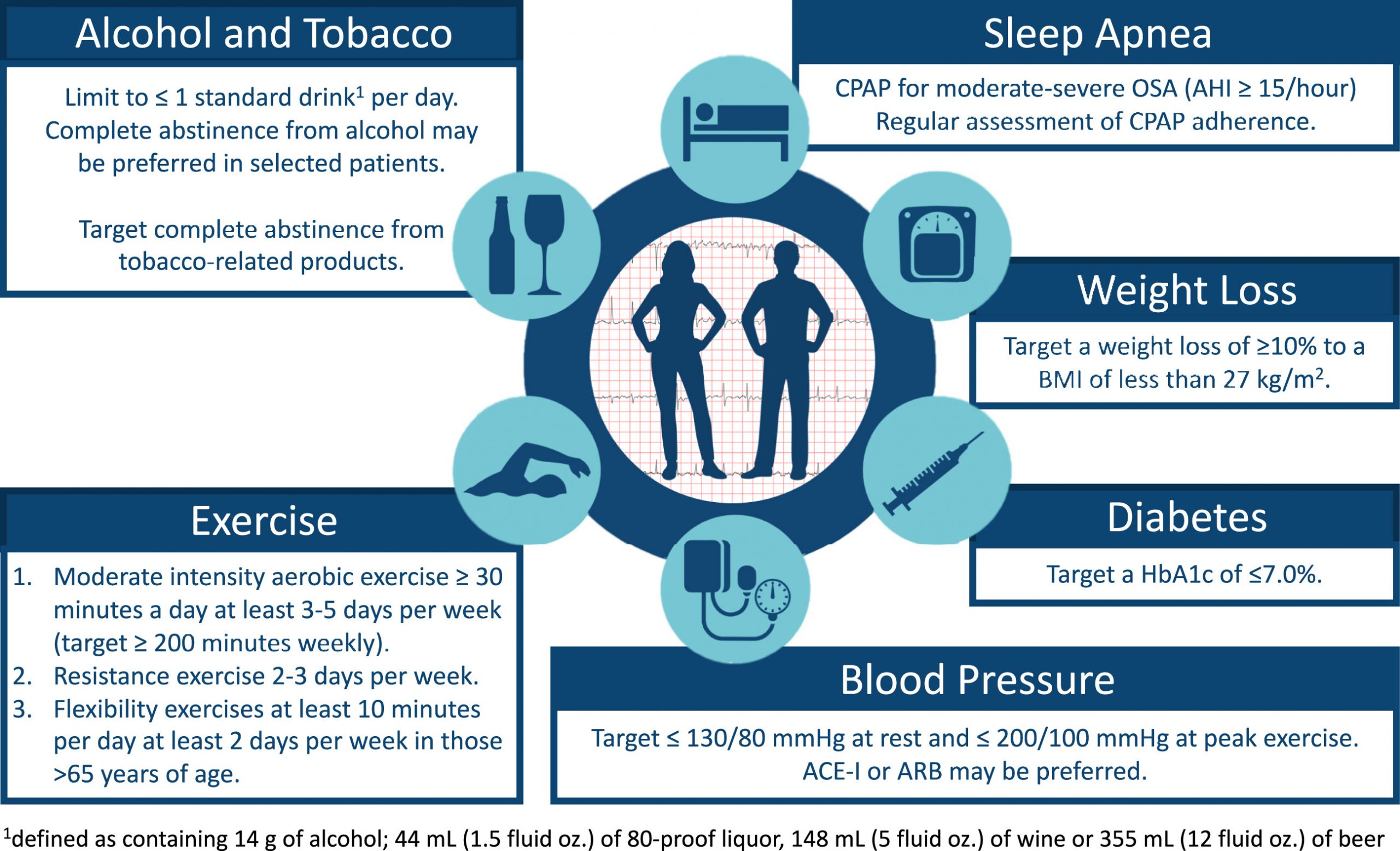
Determining the underlying cause of atrial fibrillation and modifying risk factors
Rate- or rhythm-control strategy
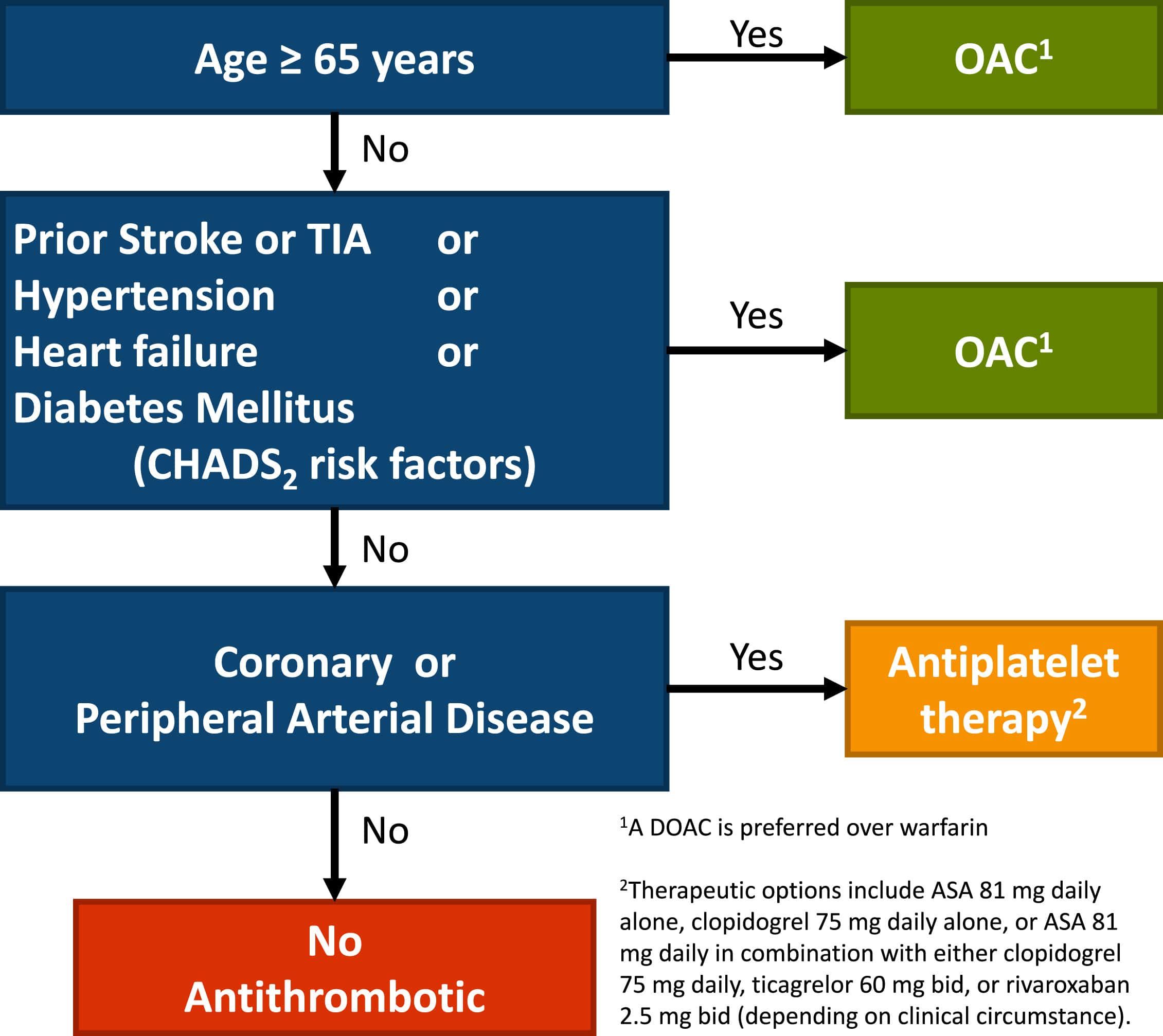
Stroke prevention (role of anticoagulation)
Definitions
Atrial fibrillation (AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation with consequent deterioration of atrial mechanical function.
On an electrocardiogram (ECG), AF is described as the replacement of consistent P waves with rapid oscillations or fibrillatory waves that vary in size, shape, and timing, and are associated with an irregular, frequently rapid ventricular response.
Irregularly irregular rhythm
Clinical classifications:
Paroxysmal AF: Continuous for >30 seconds and <7 days
Persistent AF: Continuous for > 7 days and < 1 year
Long-standing persistent AF: > 1 year and pursuing rhythm control
Permanent AF: Decision made to no longer pursue sinus rhythm restoration
Patient may have both paroxysmal and persistent episodes and should be classified based on dominant episodes
Valvular AF: Atrial fibrillation in the presence of any mechanical heart valve, or in the presence of moderate to severe mitral stenosis (rheumatic or non-rheumatic)
Important implications for anticoagulation choice
Differential Diagnosis
The differential diagnosis for tachycardia is broad. Tachycardia is usually classified based on morphology of the QRS (wide complex or narrow complex), rhythm, and presence or absence of p-waves.
Please refer to the following sites for further details:
If atrial fibrillation is due to a reversible or secondary cause, focus should be on treating the primary issue
Ie. if a septic patient develops atrial fibrillation, resuscitating the patient should be the primary goal
Patients that are hemodynamically unstable should be managed as per ACLS and undergo electrical cardioversion (see cardioversion algorithm below)
In stable patients, shared decision making to decide on acute rate vs rhythm control
Recent-onset atrial fibrillation, guidelines recommend rhythm control strategy as recent evidence suggests reduced cardiovascular death and rate of stroke (EAST-AFNET 4)
Established atrial fibrillation there is no difference in outcomes between rate and rhythm control (AFFIRM)
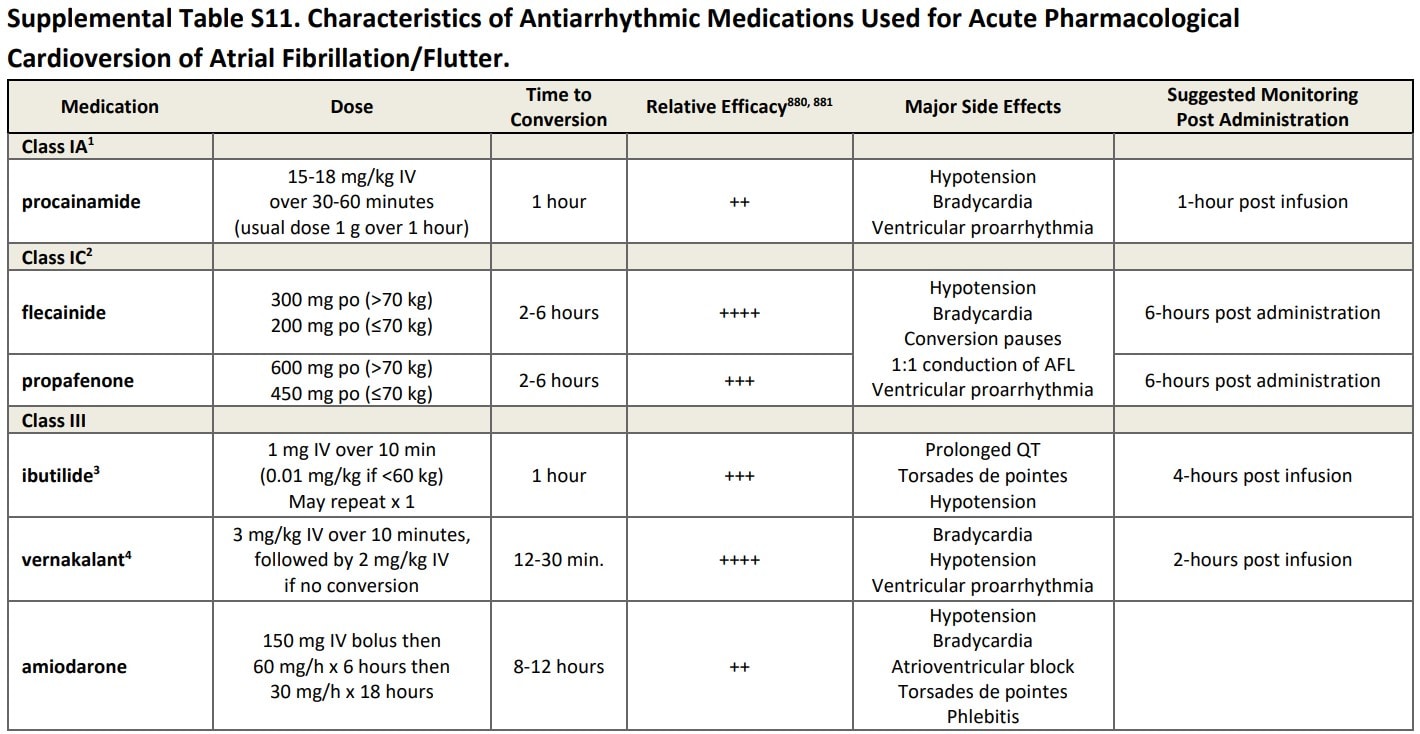
Rate control can be done with beta blockers and/or calcium channel blockers (if EF>40%) and remember to start oral meds as soon as possible after IV
CCS 2020Approach to the management of atrial fibrillation (AF) in the acute care setting
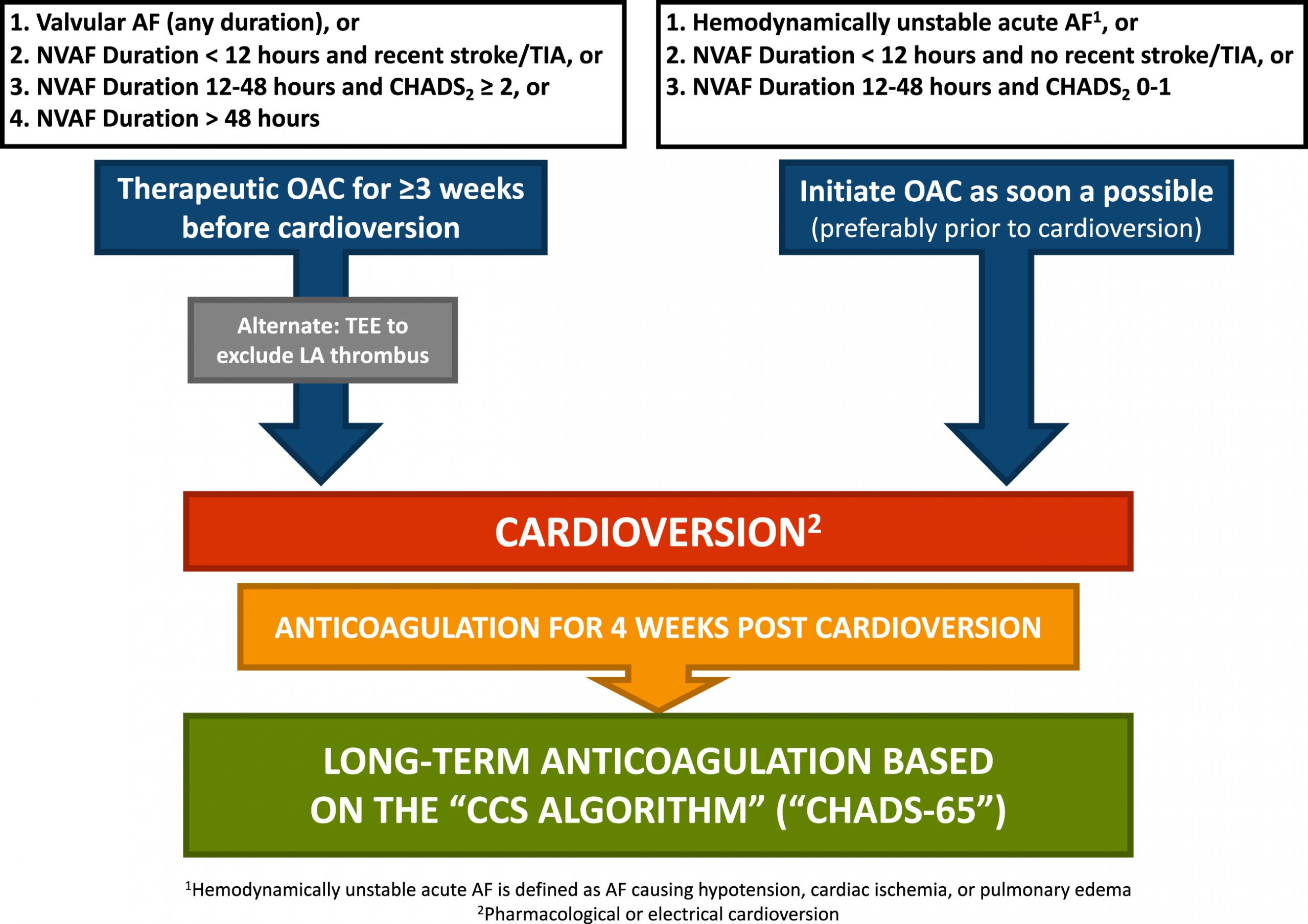
Cardioversion
Note specific duration criteria for whether cardioversion can be safely done vs needing either 3 weeks of anticoagulation vs TEE
Anticoagulation should be started as soon as possible (ideally before cardioversion)
Note: CHADS 0 patients under 65 also require anticoagulation for 4 weeks post cardioversion and everyone else long term
Recommend using max dose joules (ie. 150-200 J biphasic) to avoid repeated shocks
Pad placement (AL vs AP) does not seem to influence success)
Obese patients may require applying force over pads using paddles to improve success
CCS 2020 - Oral anticoagulation pathway in the context of cardioversion for atrial fibrillation (AF) or flutter
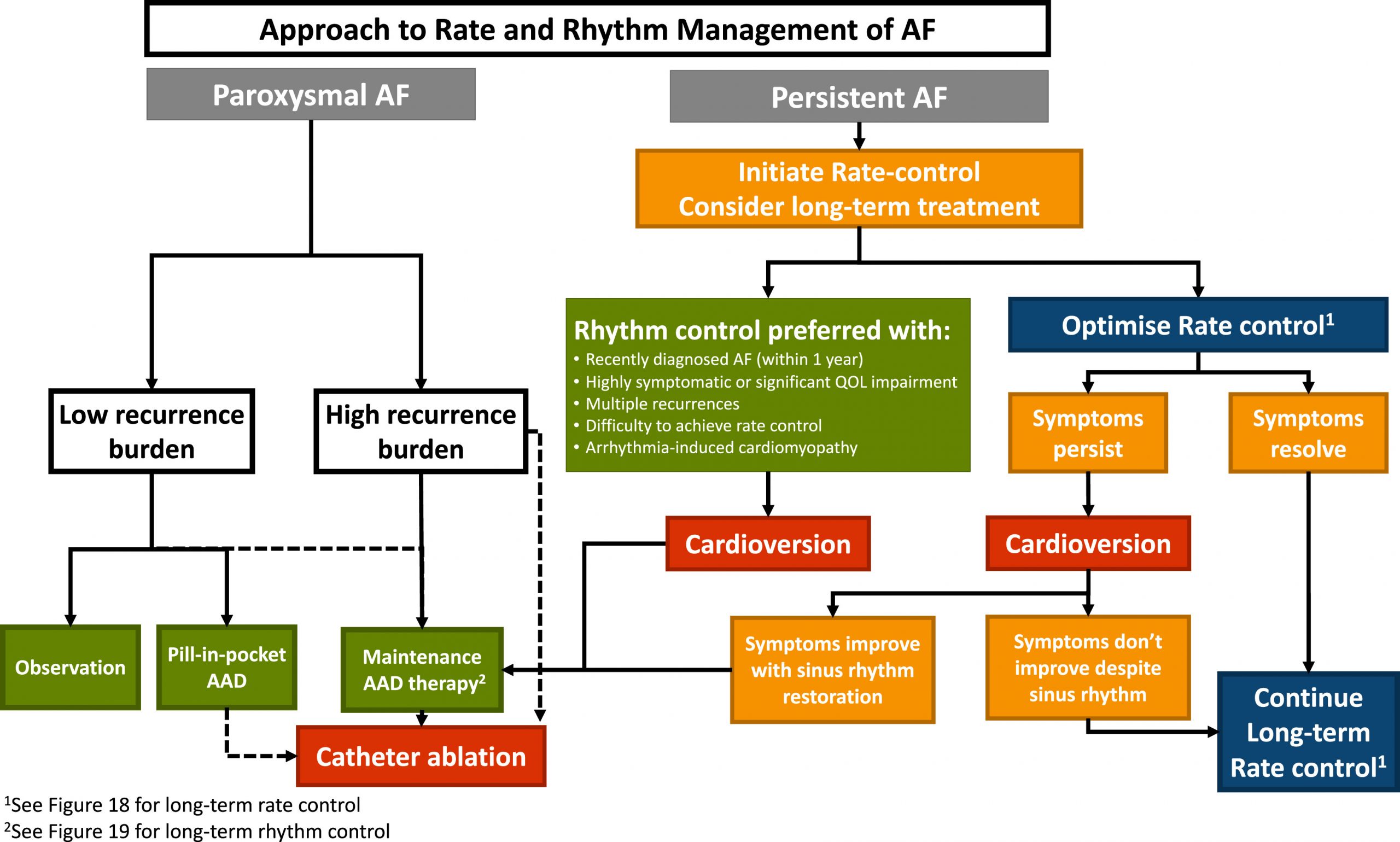
Long Term Arrhythmia Management
Approach
As above, patients with recent onset of atrial fibrillation, rhythm control strategy is a reasonable choice to prevent negative cardiovascular and stroke outcomes (especially in higher risk patients, see EAST-AFNET 4 study above)
Otherwise using both rhythm and rate control have similar outcomes and decision should be individualized to the patient.
CCS provides a framework below for how to choose strategy
CCS 2020 - Approach to rate and rhythm management of atrial fibrillation
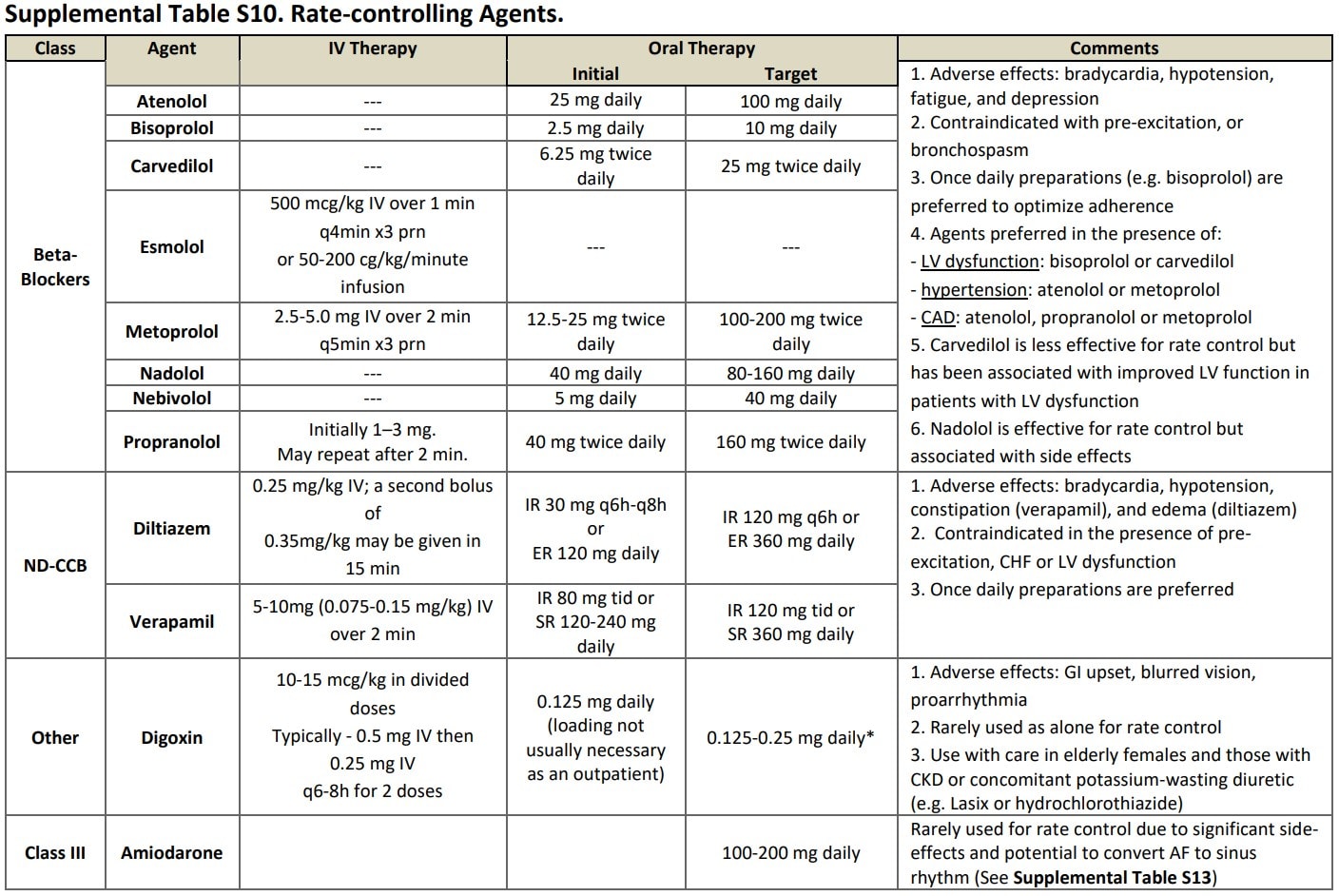
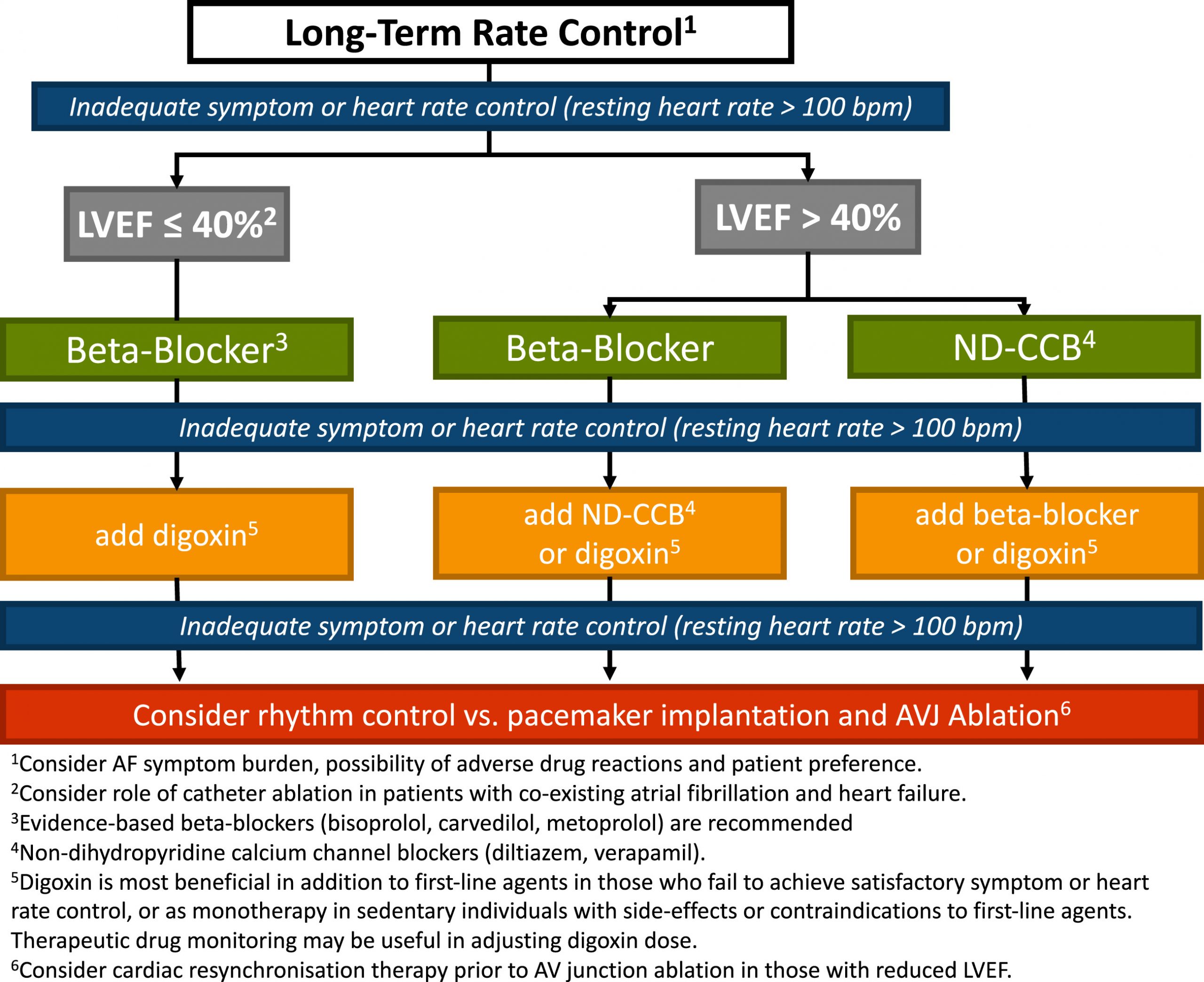
Rate-Control
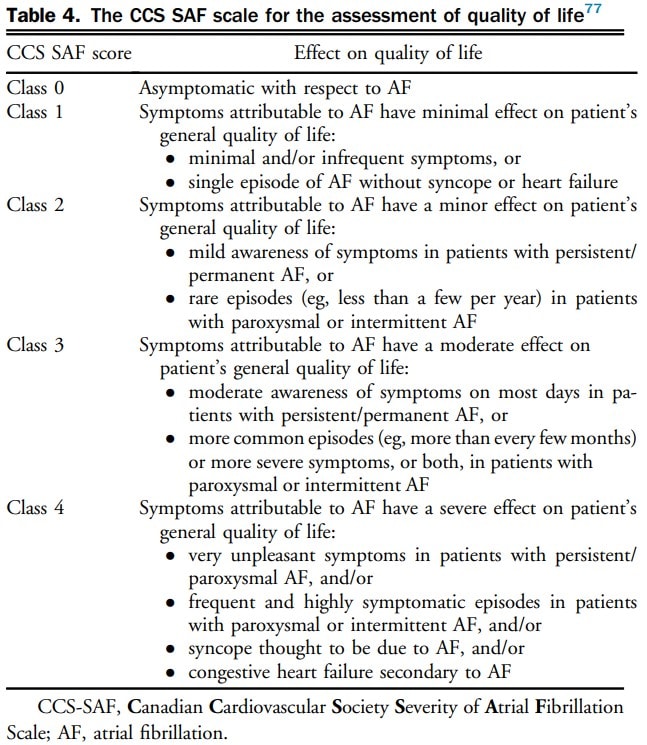
Goal is to minimize effect on quality of life
Aim for a resting heart rate of < 100 beats per minute in permanent atrial fibrillation
RACE II: Among patients with permanent atrial fibrillation, lenient rate-control (HR < 110 bpm) is as effective as strict rate-control (HR < 80 bpm) in preventing cardiovascular events
Initial therapy should be beta blockers or nondihydropyridine calcium channel blockers
Beta blockers preferred in patients with myocardial infarction or systolic dysfunction
Digoxin can be used as monotherapy in older or sedentary patients, unable to tolerate first-line medications, or as an add on if rate control target not achieved
CCS 2020 - Approach to long-term rate control
Rhythm-control
Recommended in patients who are symptomatic despite rate control, in whom rate control is thought to unlikely control symptoms, or recent onset atrial fibrillation
Rhythm control agent should be chosen based on whether they have heart failure or CAD
Pill-in-pocket strategy can be used for patients who have infrequent symptoms
CCS 2020 Approach to long-term rhythm control
Amiodarone
Acutely, IV amiodarone acts as a beta-blocker and can help rate control atrial fibrillation
Chronically, amiodarone is the most effective medications for atrial and ventricular arrhythmias, including atrial fibrillation. Patients require a total of 10 grams to saturate their tissues such that their serum levels remain high. At that point, the half-life becomes very long and it becomes an effective anti-arrhythmic medication.
Drug monitoring:
TSH ad LFTs (baseline and q6 months)
Chest Xray and ECG (baseline and q1year)
PFTs (baseline and again if symptoms)
Ophthalmic exam (if symptoms)
Catheter Ablation:
Can be used in patients who are highly symptomatic despite adequate rhythm-control trial (drug-refractory) and in whom rhythm control is desired
Can be utilized in select individuals are first line therapy (e.g. paroxysmal atrial fibrillation that is highly symptomatic) or individuals with pre-excitation atrial fibrillation with an accessory pathway
Can be utilized as first line therapy or as a reasonable alternative to pharmacologic rhythm- or rate-control therapy patients with symptomatic typical atrial flutter
Since catheter ablation is an invasive procedure, risks and benefit must be balanced
Management - Special Scenarios
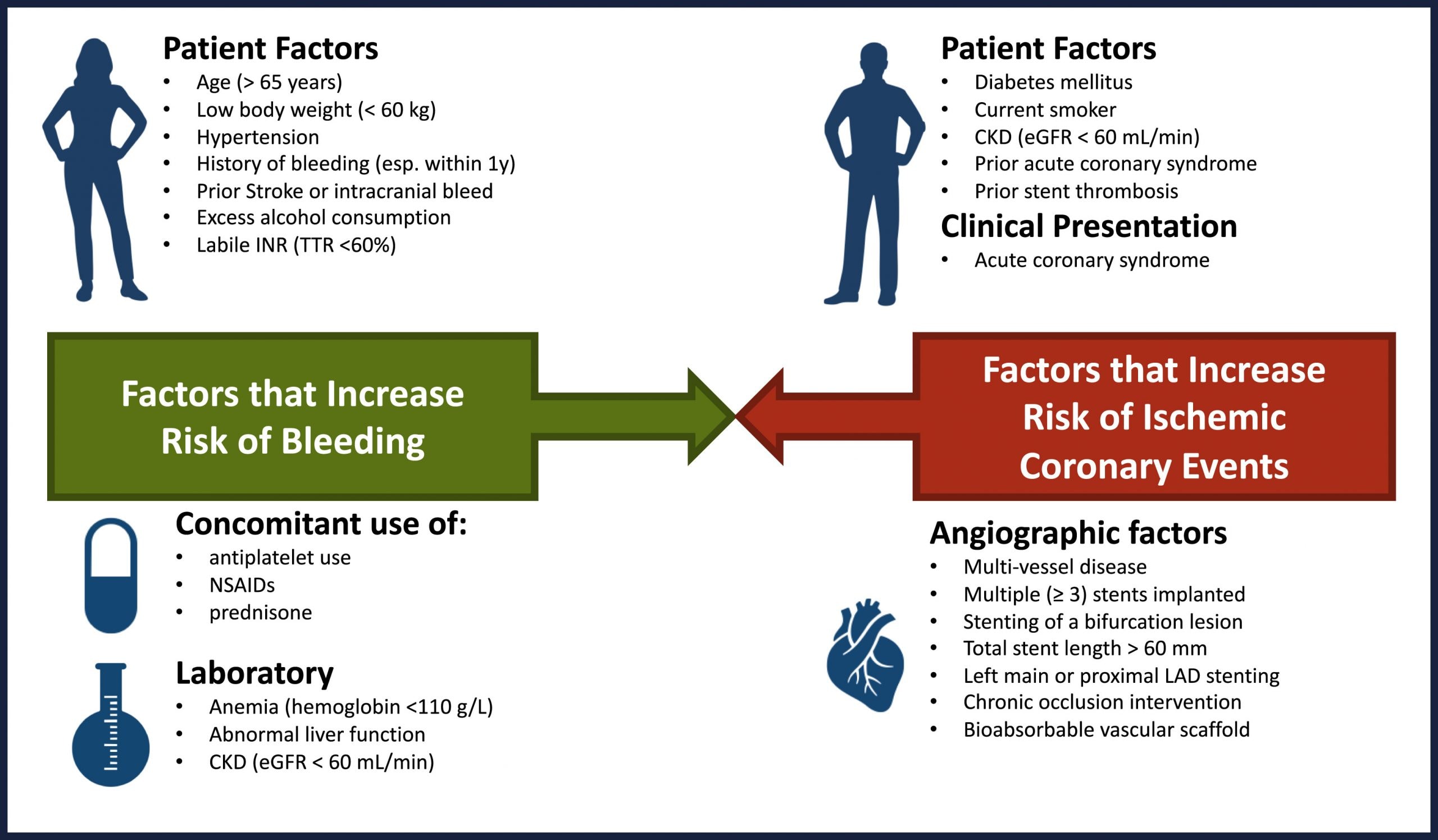
Anticoagulation/Antithrombotic Post PCI
Risks and benefits of anti-thrombotic therapy need to be balanced carefully
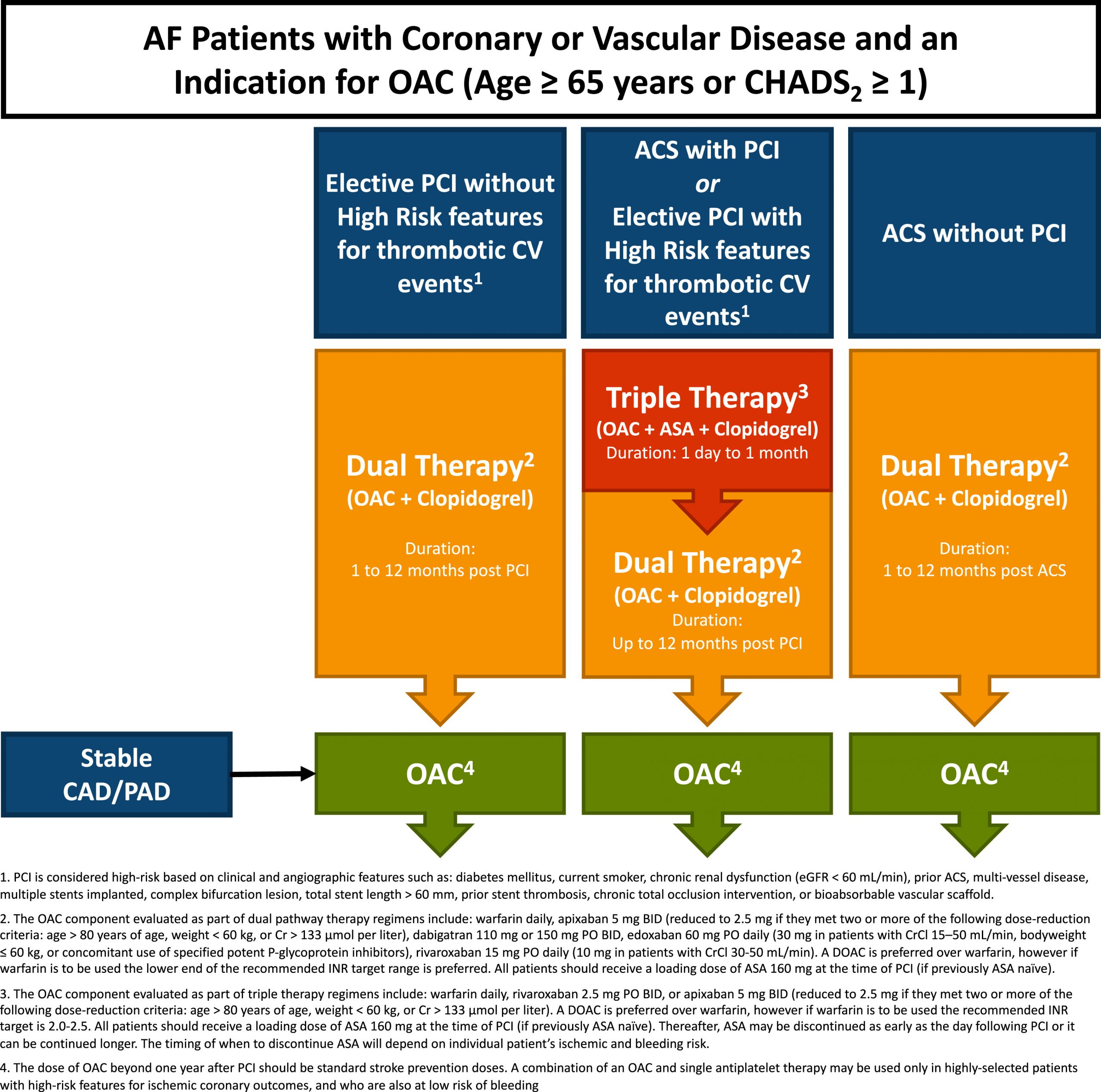
Duration of triple therapy can be decided after a discussion with the Interventional Cardiologist, who is familiar with patient’s coronary anatomy and thrombotic risk.
Generally, the duration of triple therapy is 1-3 weeks, which was the timeframe used in clinical studies.
Clinicians managing cardiac patients must be familiar with OAC management after PCI. Please carefully review the graphic titled “CCS 2020 – Management of antithrombotic and anticoagulant therapy post ACS/PCI”
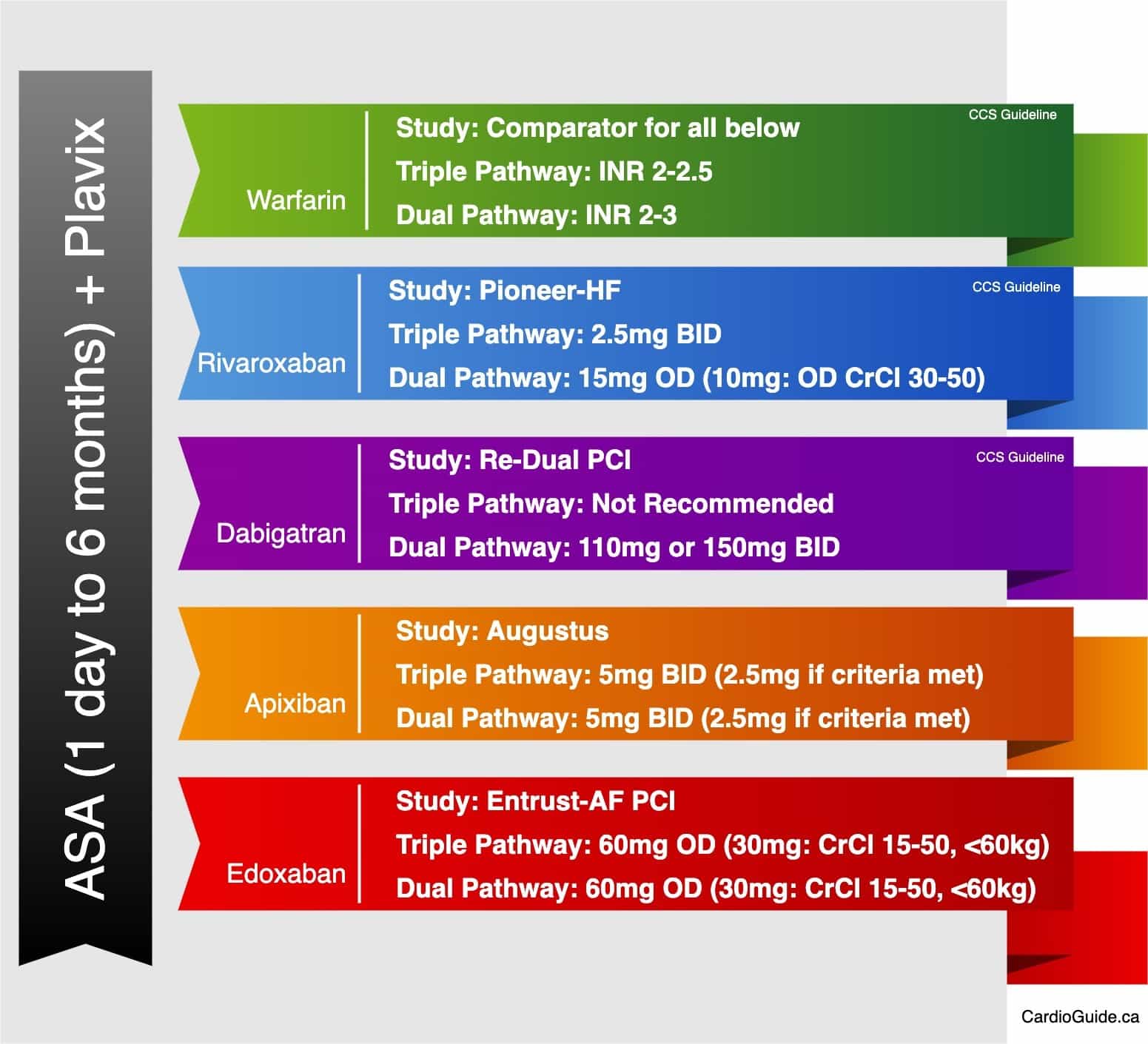
NOTE: that “Dual Therapy” and “Triple Therapy” have different OAC dosing. This was established in clinical trials.
CCS 2020 - Management of antithrombotic and anticoagulant therapy post ACS/PCI
Dosing of OAC+Antiplatelets
Peri-Operative Anticoagulation Management
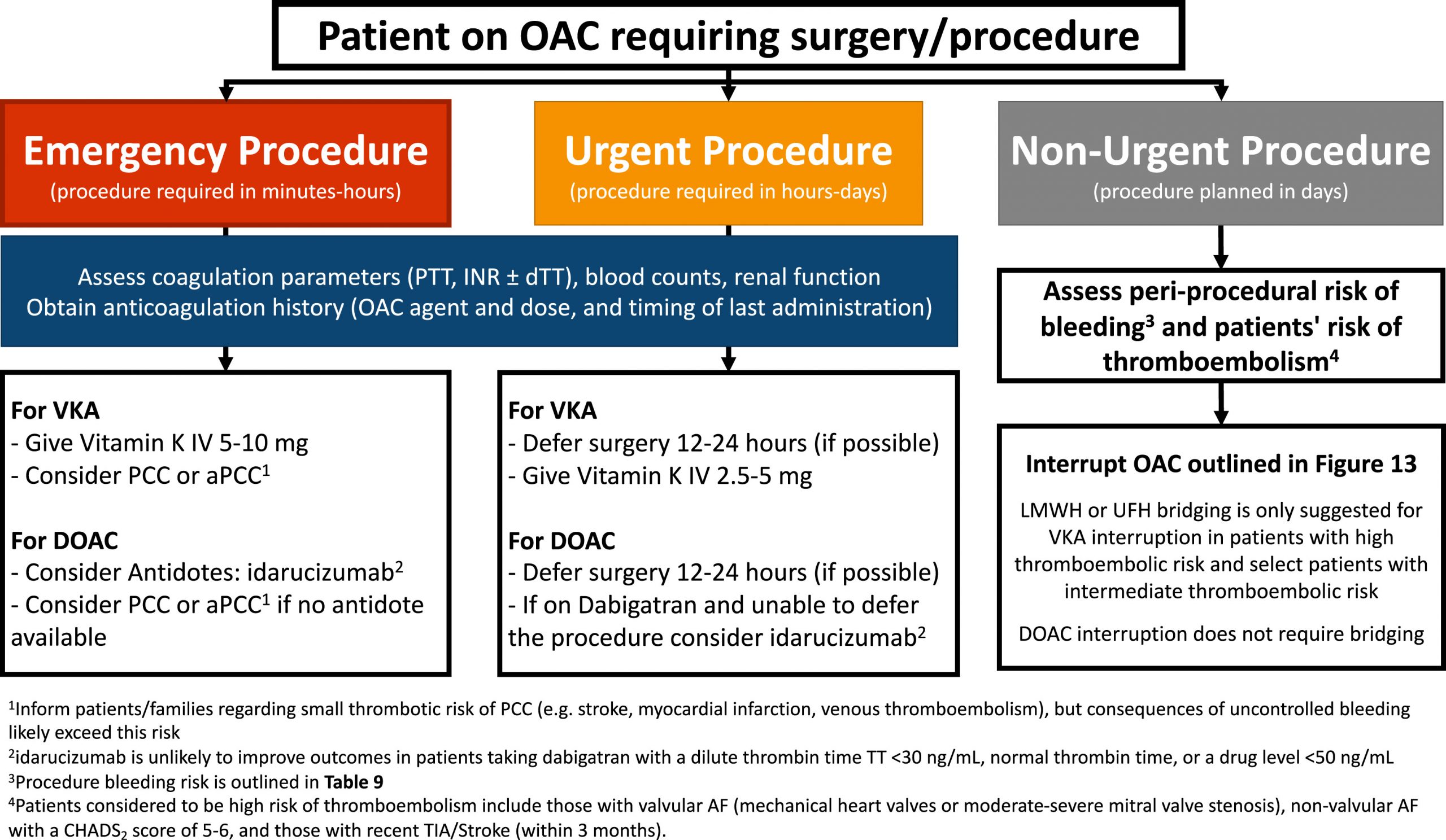
The decision to continue or stop anticoagulation should be based on risk of bleeding during procedure
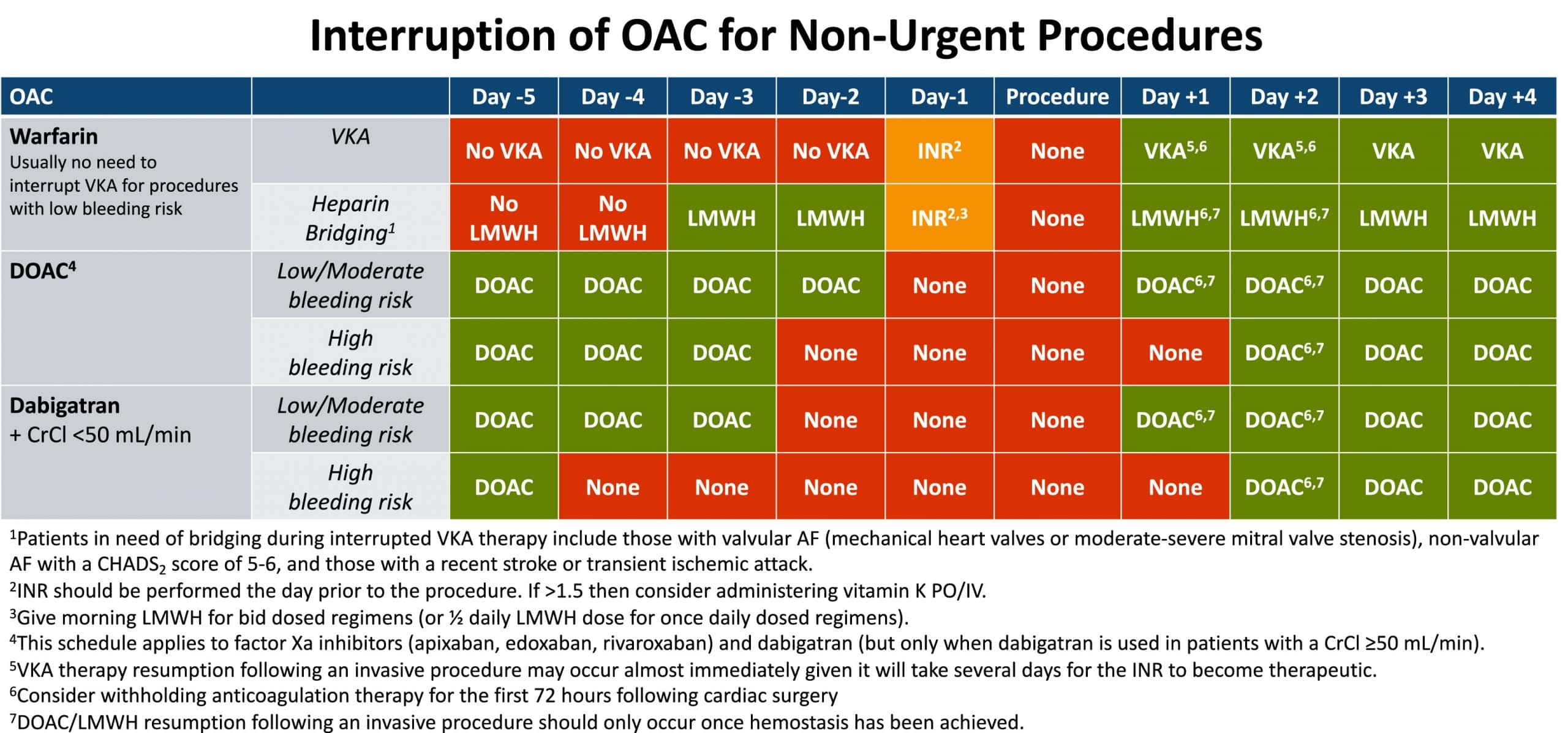
See algorithm for specific management of warfarin vs DOAC and bridging schedule
Note: DOACs do not require bridging due to short half life
CCS 2020 - Management of oral anticoagulant (OAC) use for patients requiring surgical procedures
CCS 2020 - Anticoagulation interruption schedule for patients undergoing elective or nonurgent surgery
Managing Bleeding on Anticoagulation
Management of bleeding on anticoagulation depends on the severity of bleeding and type of anticoagulant.
Note: for emergencies warfarin has multiple reversal agents, dabigatran can be reversed with idarucizumab and the anti-factor Xa (apixaban, rivaroxaban, and edoxaban) drugs can be reversed with andexanet alfa
CCS 2020 - Management of bleeding for patients receiving oral anticoagulation (OAC).
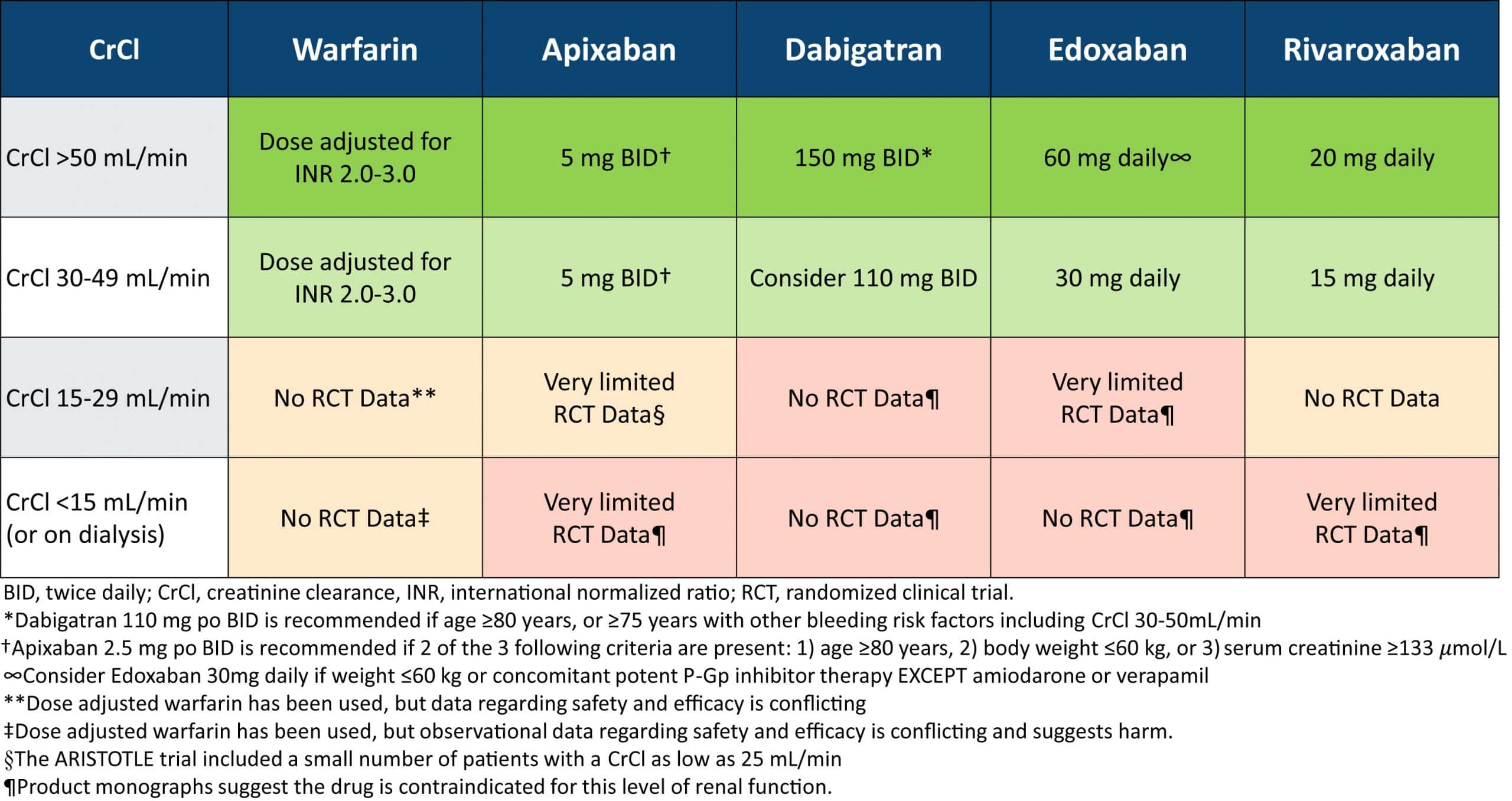
End-stage Renal Disease
CKD Stage 3 (GFR >30) and Stage 4 (GFR 15-29): anticoagulation is recommended as per CCS CHADS65 algorithm
CKD Stage 5 (GFR <15 or dialysis): guidelines recommend not routinely not performing anticoagulation but this is an area of ongoing debate
Liver Disease
Anticoagulation is not recommended for patients with Child-Pugh grade C or significant coagulopathy
Left Atrial Appendage Closure
Area of ongoing discussion but considered in patients with absolute contraindication to anticoagulant and are at risk of stroke
Can be done surgically or percutaenous
Further Reading
2020 CCS/CHRS: Comprehensive Guidelines for the Management of Atrial Fibrillation (html) (pdf)
Cardiology: A practical handbook by David Laflamme
{kind=link}
{kind=link}
{kind=link}


{kind=link}