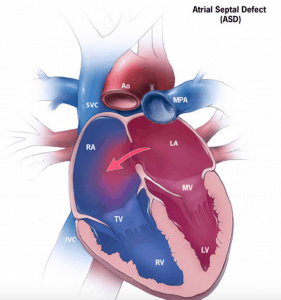
A congenital heart defect that results in a communication between the left and right atrium.
Clinical issues include exercise limitations, right heart failure, arrhythmias, stroke/TIA from paradoxycal embolism or pulmonary hypertension.
Significant ASD usually defined by an absolute size of 10mm or greater or a Qp:Qs of greater than 1.5.
CDC Public Domain Image
4 Types
Secundum: Approximately 80% found in the fossa ovale.
Primum: Second most common associated with AV canal defect.
Sinus Venosus: Involves the SVC or IVC. Usually associated with anomalous drainage of the pulmonary veins.
Coronary Sinus: A connection between coronary sinus and left atrium. Can be seen with persistent left sided SVC.
Associated Conditions
Holt-Oram Syndome: Autosomal dominant condition which affects bones and the heart. Typically assoicated with secundum ASD. Patient often have missing or abnormal upper extremity bones.
Lutembacher Syndrome: ASD with associated mitral stenosis.
Physical Exam
Fixed Split S2.
Pulmonary ejection murmur (Left-to-Right Shunt causes increase flow across the pulmonic valve.
Tricuspid regurgitation if RV failure or associated pulmonary hypertension.
Diagnosis
EKG
CXR
ECHO
EKG
RBBB
Right axis deviation
Right Atrial hypertrophy
CXR
Right Atrial dilation.
Right ventricle dilation.
Increase vascularization.
ECHO
Drop out of atrial septum on 2D echo.
Doppler evidence of shunt.
May have RV dilation of pulmonary hypertension because of left to right shunt.
Apical 4 Chamber view
Apical 4 Chamber (Zoom)
Subcostal
Subcostal Color
Apical 4 Chamber Bubble
Apical 4 Chamber Bubble with Valsalva
CAPTION
Management
Indications for closure:
Paradoxical embolism such as stroke.
Dilation of right sided chambers.
Pulmonary hypertension with fignificant shunt defined by a Qp:Qs greater than 1.5
Symptoms such as Platypnea-Orthodeoxia
Do not close if irreversible pulmonary hypertension defined systolic pulmonary artery pressure of greater than 2/3 systemic systolic blood pressure or pulmonary vascular resistance greater than 2/3 systemic vascular resistance.
Closure Strategies
Percutaneous closure can be done is the size of the ASD is less than 38 mm and the anatomy is favorable.
Surgical intervention can also be done this is especially important for sinus venosus and primum ASD as percutaneous closure generally cannot be done.
References
CCS Consensus Conference 2001 update:Recommendations for the Management of Adults with Congenital Heart Disease Part I